Download
1 / 63
630 likes | 964 Views
Adrenal masses – for Urology trainees. Ailsa Wilson, 2008. Exam questions. A fit patient is referred to you with a 4 cm incidental adrenal mass found on USS. Biochemical investigations reveal it to be non-functioning., Outline your management.

E N D
Adrenal masses – for Urology trainees Ailsa Wilson, 2008
Exam questions • A fit patient is referred to you with a 4 cm incidental adrenal mass found on USS. Biochemical investigations reveal it to be non-functioning., Outline your management. • A 42 year old woman is referred to you with a 4 cm incidental adrenal mass. How would you evaluate this lesion? • A man aged 30 with hypertension and a 6 cm adrenal mass is sent to you. Outline your evaluation.
Adrenal masses • Background: classification, incidentaloma • Adrenocortical carcinoma • Relevant endocrine pathways and syndromes: hyperaldosteronism, glucocorticoid excess, phaeochromocytoma • Investigation: • Radiology • Endocrine • Management: • Surgical (and preoperative management) • Medical
Adrenal masses • Adrenocortical masses are common • O.4-6% Of CT Scans • 6.5-8.7% Of Autopsy Series • “incidentaloma”: any adrenal mass discovered by noninvasive abdominal imaging performed for reasons other than suspected adrenal disease • retrospectively often found to have had symptoms or signs related to an adrenal tumour • Incidence Increases With Age; < 1% under 30 y, 7% After 70, and as imaging increases • More Commonly In Women • Less commonly, adrenal masses are identified in workup for suspected adrenal disease • 80% adrenal masses are nonfunctioning and benign • 20% are functioning • 0.1-1% of total are malignant
Adrenal masses • Main concerns with an adrenal mass are • (1) whether it is malignant • -> identify early and attempt surgical cure/directed treatment if secondary • (2) whether it is hormonally active • -> treat appropriately (surgical/medical)
Classification adrenal masses • Benign • Adenomas • Functional vsNonfunctional • Haemorrhage, TB, fungal (systemic diseases that can produce adrenal insufficiency) • Malignancies • Adrenocortical carcinomas • Functional vsNonfunctional • Well differentiated vs Intermediate vs Poorly differentiated to anaplastic • Metastatic: Most commonly: Lung , Breast , Melanoma , RCC • Adrenomedullarytumors • Malignant phaeochromocytoma • Ganglioneuroblastoma • Neuroblastoma • Neuroendocrine carcinoma • Stromal malignancies : Neurofibrosarcoma ,Angiosarcoma ,Liposarcoma ,Fibrosarcoma , • Composite or mixed tumors: rare, ie, coexisting neuroblastoma and malignant phaeo • familial predisposing syndromes : Li-Fraumeni, MEN-1, Beckwith-Wiedemann
Prevalence of adrenal incidentaloma • Non-hypersecretory adrenal adenoma 74-85% • Hypersecretory tumours • Cortisol secreting adenomas 9.2% • Phaeochromocytomas 4.2-10% • Aldosteronomas 1.4% • Androgen/estrogen secreting • Primary adrenal carcinoma 0.1-4% • Other adrenal masses • Myelolipoma 3-10% • Cysts 1.9-10% • Ganglioneuromas 1.5% • Haemorrhage, TB, fungal • Metastases 0.7-30% • ¾ of lesions found in patients with cancer are metastatic • 2/3 of masses in patients without a cancer diagnosis are benign • The incidental adrenal mass. Am J Med 1996
1. Is it malignant? Adrenocortical carcinoma Metastases to the adrenal
Adrenocortical carcinoma • Uncommon: 0.6-1.67 cases/million/per year. • Important to distinguish potential carcinomas from other masses • female-to-male ratio 2.5-3:1. • Male -older , worse overall prognosis than female • Female -more likely to have an associated endocrine syndrome. • Nonfunctional ACs distributed equally between sexes. • 2 peaks: first decade of life and again in the fourth to fifth decades. • Most sporadic and unilateral • 2% to 6% are bilateral -associated with Li-Fraumenisynd, MEN-1, Beckwith-Wiedemannsynd, and Carney complex primarily in children • pathogenesis of sporadic AC unclear
Adrenocortical carcinoma • Nonfunctional 40% • ?progress more rapidly • fever, LOW, abdo pain (infiltration, haemorrhage, necrosis), fullness, back pain, Sx related to mets or incidental finding • Functional ?60% • Detected earlier • Difficulty in discriminating adenoma from carcinoma on histology (Weiss criteria 1984) • Not all large adrenal lesions behave like carcinomas. • Some lesions that appear benign on histologic evaluation eventually metastasize. • -> FNA not useful in workup
Complications of adrenal carcinoma • Complications • Local invasion, tumor thrombus can embolize similar to RCC • Hormone excess syndromes (Cushing syndrome, hyperaldosteronism, hirsutism, virilization, and hypertension) • Paraneoplastic syndromes (cachexia) • painful bone metastases • Prognosis: functional may have a better prognosis because present earlier • Poor overall 5-year survival 20-35%. • total surgical resection -> 32-47%, ?up to 70%. • Even after complete surgical resection, risk of local or distant relapse is 80% • total surgical resection not been possible-> 10-30%. • distant metastasis: 50% are dead within 12 months, 5 y survival 5%
Staging for adrenal carcinoma • Sullivan et al • Tumor criteria • T1 - Tumor diameter smaller than or equal to 5 cm with no local invasion • T2 - Tumor diameter larger than 5 cm with no local invasion • T3 - Tumor of any size with local extension but not involving adjacent organs • T4 - Tumor of any size with local invasion of adjacent organs: kidney, liver, tumour extension into venous drainage of adrenals and IVC • Lymph node criteria • N0 - No regional lymph node involvement • N1 - Positive regional nodes • Metastasis criteria • M0 - No distant metastasis • M1 - Distant metastasis: most common sites lungs, liver, bone, and lymph nodes. • Stages • Stage 1 - T1, N0, M0 • Stage 2 - T2, N0, M0 • Stage 3 - T1 or T2, N1, M0 • Stage 4 - Any T, any N + M1 or T3, N1 or T4
Adrenal metastasis • More common than primary adrenal carcinoma • >50% of patients with melanomas , breast, lung; • 40% of patients with RCC • Also contralateral adrenal, lymphoma, leukaemia, TCC, colon, esophagus, GB, liver, pancreas, prostate, stomach, uterus • Now identified earlier in the course of patients with cancer • Distinguishing a metastatic lesion from a primary: • Majority has history of malignancy and multiple mets • Nonfunctional • MRI pattern characteristic • FNA controversial- indicated when metastatic disease is likely, and detection would alter management.
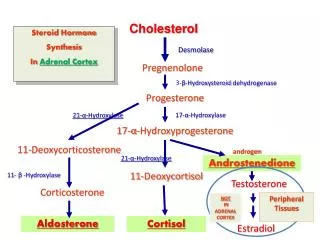
Physiology: Cortex 3 zones • ZG: mineralocorticoids • Small cells with intermediate number of lipid inclusions • ZF: glucocorticoids • Large foamy cells (lipid inclusions) • 75% of cortex • Glucocorticoids are essential for life • ZR: adrenal androgens • Compact cytoplasm, few lipid inclusions
Physiology: Adrenal Cortex • common precursor used to produce series of steroid hormones • Rate limiting step for all is production of pregnenolone from cholesterol • H-P-A regulation is complex
Functional tumours • Elaborate adrenal hormones (glucocorticoids, mineralocorticoids, androgens, estrogens, many other possible peptides). • Evidence of hormonal excess includes: • Cushing syndrome for cortisol-secreting adenomas • Hypertension and hypokalemia for hyperaldosteronism • Labile hypertension and spells for pheochromocytoma • Virilization in women for androgen-secreting tumors • Feminization in men for estrogen-secreting tumors
Physiology: Cortex - Glucocorticoids • Control: CRH->ACTH • ant pituitary • precursor: proopiomelanocortin, also makes MSH • diurnal • 90-95% of circulating cortisol is protein bound • 7%-10% free (metabolically active) • variations in binding proteins influence total plasma cortisol value but not free cortisol
Physiology: Cushing’s syndrome • symptom complex caused by excess circulating glucocorticoids • Includes: • Cushing's disease (pituitary adenoma) 70-85% • adrenal adenomas 10% • Adrenal carcinomas 8% • Micronodular hyperplasia <1% • Macronodular hyperplasia <1% • Ectopic secretion of ACTH or CRH 12% • Pseudo–Cushing's • Major depression<1% Alcoholism <1% • Exogenous steroids (most common) • Orth DN: Cushing's syndrome. N Engl J Med 1995;332:791.
Cortisol secreting incidentalomas • Most common incidental secreting mass (5-15%) • in one study of patients with incidentalomas, 24% were found to have subclinical Cushing's syndrome. • metabolic syndrome: obesity, hypertension, dyslipidemia, impaired glucose tolerance. • may have reduced bone density and osteoporosis. • Clinical features improve after adrenalectomy • If not removed the endocrinopathycontinues • Up to 50% of incidentalomasmay have one /more slight abnormalities of H-P-A axis • (high-borderline urinary free cortisol, impaired cortisol rhythm, only partial cortisol suppression with dexamethasone, low plasma ACTH, unresponsiveness to CRH) • Adrenal insufficiency after removal of “silent” adenomas in up to 20% • Coricotrophin suppression and atrophy of contralateral gland • Partial suppression can persist for several months after adrenalectomy. • May require perioperativeglucocorticoids
Physiology: Cortex - Aldosterone • Control: R-A-A, sensor in JG apparatus • main stimulus is reduced renal perfusion, renin release, • Sodium retention to attempt to restore renal perfusion • accompanied by water so isotonicity is maintained • usually gradual. Mineralocorticoid escape. • Plasma potassium also controls aldosterone release (blunted by hypokalaemia) • can result in lowering of plasma aldosterone to normal range in patients with hypokalaemia and hyperaldosteronaemia • poorly bound to albumin and plasma protein • half-life 20-30 minutes.
Aldosterone producing adenoma • Rare • Most common cause of hyperaldosteronism • Twice as common in women • Mean 30-50 y • Mostly unilateral • Mostly < 2 cm • Conn (1955)—First curative treatment of APA by unilateral adrenalectomy • Difficult to control HT • Headache • Weakness/ Fatigue • Paraesthesia • Muscle Cramps • Polyuria/ Polydipsia • Arrhythmias • Hypokalemia • Metabolic Alkalosis • Hyperaldosteronism • Hyporeninemia
Physiology: Adrenal Androgens (DHEA) • Control: ACTH and other mechanisms • Peripheral conversion of DHEA to DHEAS • some diurnal variation. • weakly active, in contrast to testosterone, appear relevant only in pathologic states (CAH) • not produced in significant quantities by other tissues (except occ PCOS, gonadal tumours) • Virilisation: • 5% of women with hirsutism will have have a significant adrenal pathologic process • Patients with high DHEA also have high 17-ketosteroids, virilizationcaused by elevated testosterone does not. • Elevated DHEA, androstenedione, or 17-ketosteroids out of proportion to glucocorticoids suggest adrenal carcinoma • feminisation 6%: • Virtually all feminizing adrenal tumors in men are highly malignant • gynaecomastia, infertility, low libido • Androstenedione converted peripherally to estrogens Rare as incidentalomas Many are malignant
Physiology: Adrenal medulla • chromaffin cells secrete primarily adrenaline (also noradrenaline, dopamine) • PNMT catalyzes methylation of Nad -> Ad, almost localized to the medulla • high levels of glucocorticoids are necessary to maintain high levels of PNMT and Ad secretion -> location of the adrenal medulla • dietary tyrosine and phenylalanine are substrates • Catecholamines stored in vesicles • Stimulation of preganglionic sympathetic nerves (stress, pain, cold, heat, asphyxia, hypotension, hypoglycemia, and sodium depletion) -> exocytosis
Physiology: Adrenal medulla • plasma half-life <20 sec • Neuronal reuptake for re-release, or degraded by COMT and MAO • primary metabolite in the urine is vanillylmandelicacid • metanephrine, normetanephrine, and their derivatives contribute to total metabolic products
Physiology: Adrenal medulla • Catecholamines exert varied effects by stimulating adrenoreceptors • diversity of effects accounts for the diversity of symptoms in pheochromocytomas. • different tumors produce different proportions of Nad, Ad, or dopamine. • if there is excessive production of both Nad and Ad, the lesion is almost always within the adrenal, not other sites of chromaffin tissue.
Phaeochromocytoma • 1 in 1000 autopsies. 1-10% of incidentalomas • more common than previously thought, failure to recognize may lead to death. • Assume adrenal adenomas are phaeochromocytoma until proven otherwise • Noradrenaline secretion most common • Paroxysmal hyperadrenergicSx: headaches (80%), palpitations (64%), sweats (57%), abdominal pain. • Hypertension: Paroxysmal 48%, Persistent 29%, Normal 13% • 1981 Sutton: 25% of phaeochromocytomas found postmortem were not diagnosed antemortem (20-80% in other series) • 90% of these patients had characteristic symptoms. • Many died of causes possibly related to phaeo. 29% died unexpectedly during surgery, 27% died from cardiovascular causes, 17% died from cerebrovascular causes. • Not possible to determine the malignant potential of pheochromocytoma
Functional adrenal carcinoma • Most secrete multiple compounds or nonfunctional/small volume metabolites • 50-80% are functional, especially in children • Adults: • 30-40% present with typical Cushings, • 20-30% present with virilization (overlap) – “Virilisation is the hallmark of Cushings due to carcinoma” • feminisation 6%: • aldosteronism2.5%, catecholamine excess similarly rare. • Combined hormone excess (35%), Polycythemia ( <1%), Hypercalcemia ( <1%), Hypoglycemia ( <1%) • Children: >80% present with virilization(precocious puberty) (isolated Cushings only 6%) • Ng L, Libertino JM: Adrenocortical carcinoma: Diagnosis, evaluation and treatment. J Urol 2003;169:5-11.
Is an extensive diagnostic workup justified (discomfort, cost) in this particular patient?
Investigation • Agreement that all patients with solid adrenal masses should undergo biochemical assessment. • If biochemical abnormalities identified, lesions should be treated—usually by removal • A selective approach limits cost without sacrificing diagnostic accuracy. • History and examination • CT/MRI • Serum and urinary cortisol (24h) to screen for Cushing's syndrome; • urine or plasma metanephrine, VMA determinations to screen for phaeochromocytoma; • (?in patients with hypertension only), serum potassium concentration and plasma renin-to-aldosterone ratio. • test recommendations have expanded since 1990 following the demonstration of more subclinical hormonal abnormalities.
Investigation of adrenal masses • History • Endocrine Sx: weight gain, weakness, depression, and bruising, GI Sx • Phaeochromocytoma: episodic headaches (80%), palpitations (64%), sweats (57%), abdominal pain. • Hirsutism/feminisation, oligo/amenorrhea, and increased libido • Children: precocious puberty, weight gain, growth retardation • Malignancy: weight loss, fever • PMHx: difficult to control hypertension • Surgery • Other malignancy • CV disease, osteoporosis, obesity, diabetes • Medications: exogenous steroids, multiple antihypertensives
Investigation of adrenal masses • Examination • Abdominal/flank mass • Hyper/hypotension, postural hypotension, tachycardia • Weakness, ileus • Truncal obesity, supraclavicular and dorsocervical fat pads, gynaecomastia, proximal muscle wasting • Hirsutism, facial acne, striae, malar flushing • virilization in girls, or precocity and feminization (rarely) in boys. • Fundi: hypertensive retinopathy. • Hypo/hyperglycaemia • ectopic ACTH: cachexia, hypertension, skin pigmentation, hypokalemic alkalosis • Old photographs
Imaging • CT and MRI: imaging of choice • USS • Scintigraphy • PET • Angiography, venography
CT • size, shape, appearance. • Targeted CT with 3-5-mm sections give best resolution esptumors ≤1 cm • Smooth, homogeneous solitary lesion <4 cm with low attenuation ie lipid rich (<10 HU) is usually benign. • Look for atrophy of the opposite gland • red flags for a possible carcinoma/metastasis • Irregular • Large size (>4 cm) • calcification • heterogeneity on plain and contrast (?intralesionalhemorrhage/necrosis) • High attenuation values (>20 HU) • invasion of local structures or extension into major vessels • lymphadenopathy • large adenomas (≥5 cm ) often share features of carcinoma
Bilateral adrenal hyperplasia Adrenal adenoma
MRI • as effective as CT for distinguishing benign from malignant • superior for detecting phaeochromocytomas. • nonfunctionaladenoma has a T2-weighted intensity similar to liver tissue, mild-no enhancement, rapid contrast washout. • Malignant: intermediate-to-high density on T2 imaging, rapid and intense enhancement with gadolinium contrast, with sluggish washout. • Haemorrhage, metastases and neural tumours also high density on T2 • pheochromocytomas: very high signal intensity.
MRI R adrenal ca, T1 weighted image T2 weighted image – signal intensity much higher than liver or spleen
Functional nuclear imaging (scintigraphy) • For lesions not adequately characterised with CT and MRI. • Not widely available, usefulness limited • [(131)I]-6-iodomethyl norcholesterol (labelled cholesterol analogue) • ?can differentiate functional adrenal cortical adenomas or functional adrenal tissue from other retroperitoneal lesions • rarely indicated in suspected AC • [(123)I]- and [(131)I]-meta-iodobenzylguanidine (labelled noradrenaline analogue) – abnormal/increased uptake in phaeochromocytomas • Excludes extraadrenal/bilateral phaeos
PET and other • PET: variety of agents • can discriminate between cortical lesions and either metastatic disease or neural tumors but not between benign and malignant cortical tumors • Arteriography and venography currently have little use in diagnostic evaluation • adrenal venous sampling ie to demonstrate bilateral/unilateral hormone secretion preop • USS: less sensitivity in detecting adrenal tumors , user-dependent , Good for follow-up
Hormonal workup • Initial screening: • Electrolytes: K+, Cl-, Ca2+, Na+, creatinine • Serum aldosterone and reninto compute aldosterone-to-reninratio • DHEA, testosterone • 24-hour urinary cortisoland creatinine for cortisol excretion. • 24-hour urinary catecholamines (epinephrine, norepinephrine) and metabolites (VMA, metanephrines and normetanephrines) • And then if indicated: • Low dosedexamethasone suppression test, • Serum ambulatory cortisol, ACTH • Urinary free cortisol, high dose dexamethasone suppression, others • Other serum adrenal androgens (androstenedione), 24-hour urinary 17 ketosteroids. • +/-Plasma estradiol and/or estrone, 17-hydroxyprogesterone • Urinary metanephrine-to-creatinine ratio, plasma metanephrines and catecholamines • Ross NS. Hormonal evaluation of the patient with an incidentally discovered adreanl mass.EJM 1990:323:1401-1405
Glucocorticoids • establish the presence of Cushing's syndrome and to distinguish between pituitary and adrenal causes and ectopic ACTH secretion • 24-hour excretion of cortisol in the urine is the most direct and reliable • (2/3 consecutive specimens) • If normal in three collections, Cushing's syndrome is unlikely • Mildly elevated in anxiety, depression, alcoholism
Glucocorticoids • Next test is the low dose dexamethasone suppression test • exclude Pseudo-Cushings or Dx subclinical Cushings • 0.5 mg orally 6 hourly for 2 days OR single 1 mg dose in evening, measure in morning • Normal: fall in plasma cortisol (<5 ng/dL) or other measures • Cushing's syndrome: resistance to suppression • Usually reserved for patients with equivocal 24-hour urinary cortisol • OR use am and pm plasma cortisol and ACTH levels . • determine the presence/absence of the normal circadian rhythm • Normal rise in morning plasma cortisol with a fall to <5 ng/dL in the evening – lost in Cushing's syndrome (or show some variations at higher basal levels) • plasma cortisol >50μg/dL and ACTH suppressed<5pg/mL=ACTH independent (primary adrenal Cushings) • plasma ACTH >50 pg/mL, the cortical secretion is ACTH dependent (pituitary or ectopic ACTH/CRH)
Glucocorticoids • high-dose dexamethasone suppression test has been the standard to differentiate pituitary vs adrenal Cushing's. • dexamethasone (2 mg every 6 hours for 2 days), measure plasma cortisol, urinary free cortisol • pituitary disease,: 50% or greater suppression in cortisol. • adrenal adenomas or carcinomas :fail to suppress cortisol secretion. • Urinary free cortisol is also used as in screening (Elevated in 3.3% of lean, obese, or chronically ill patients) • late-night salivary cortisol concentration - high sensitivity, specificity • Additional tests to differentiate between pituitary overproduction ACTH (Cushing's disease) and ectopic ACTH secretion • metyraponestimulation tests • petrosalvenous sinus catheterization. • Imaging for occult ACTH-secreting tumors: CT/MRI, radionuclide imaging for somatostatinreceptors (small cell lung ca and thymic carcinoid) • CT or MRI of the sellaturcica
Subclinical Cushings in incidentalomas • Because urinary free cortisol levels may be within the reference range, a dexamethasone suppression test may be needed to diagnose • some centres perform more in-depth testing (diurnal rhythm evaluation with 8 am and midnight serum or salivary cortisol estimations, CRH stimulation test, serum ACTH (generally low), and serum DHEAS (generally suppressed))
Testing for primary hyperaldosteronism • *Aldosterone/PRA Ratio • ideally upright • Normal < 20 • Primary Aldosteronism> 30 (with suppressed plasma renin level and plasma aldosterone concentration >0.5 nmol/L) • > 90% Sensitivity And Specificity • aldosterone will not rise with ambulation • aldosteronenot suppressed by sodium loading (Saline Infusion test) or fludrocortisone • Urinary aldosterone excretion considered accurate also • to distinguish adenoma from idiopathic hyperaldosteronism(25%: bilateral adrenal hyperplasia) • Radiological appearance • Adrenal venous sampling - lateralisation • 18-OH-Corticosterone • Adenoma if >100 mg/dl -> surgery • hyperplasia if <50 ng/dl -> spironolactone • NATIONAL INSTITUTES OF HEALTH Management of the Clinically Inapparent Adrenal Mass (Incidentaloma). Final Statement. 2002
Testing for androgen overproduction • Of tests of adrenal androgen function • plasma DHEA/DHEAS is more commonly used and is more accurate than androstenedionevalue. • serum testosterone • Plasma estradiol and/or estrone, 17-hydroxyprogesterone, • 24-hour urinary 17 ketosteroids.
Testing for phaeochromocytoma • Urine and Plasma collection of catecholamines and metabolites • metanephrines, vanillylmandelic acid (VMA), and fractional catecholamines • Plasma free metanephrines preferred in some centres • Which Is Better? • Series of catecholamine-secreting tumors in 31 of 340 patients: • Plasma free metanephrine sensitivity 97%, Specificity 98% • Urinary total metanephrine and catecholamines sensitivity 90%; Specificity 85% • NATIONAL INSTITUTES OF HEALTH Management of the Clinically Inapparent Adrenal Mass (Incidentaloma). Final Statement, 2002 • Sawka et al. JCEM 88(2): 553-558. 2003.?
FNA/core biopsy • Can’t reliably distinguish adenoma from carcinoma • histologic analysis may be unreliable, • potential for tumor seeding into the retroperitoneum. • “no role in the diagnostic workup of adrenal incidentalomas” • Generally not recommended except for possible metastatic deposits/lymphoma. • Never perform FNA without first excluding phaeochromocytoma