Download
1 / 1
10 likes | 61 Views
Readmission After Heart Failure Hospitalization in Alberta, Canada 2004-2010 Cathy A. Eastwood, RN, MN 1 ; Alka Patel, PhD 2 ; Jonathan Howlett , MD 3 ; Kathryn King-Shier, RN, PhD 1 ; Hude Quan , MD, PhD 2. BACKGROUND

E N D
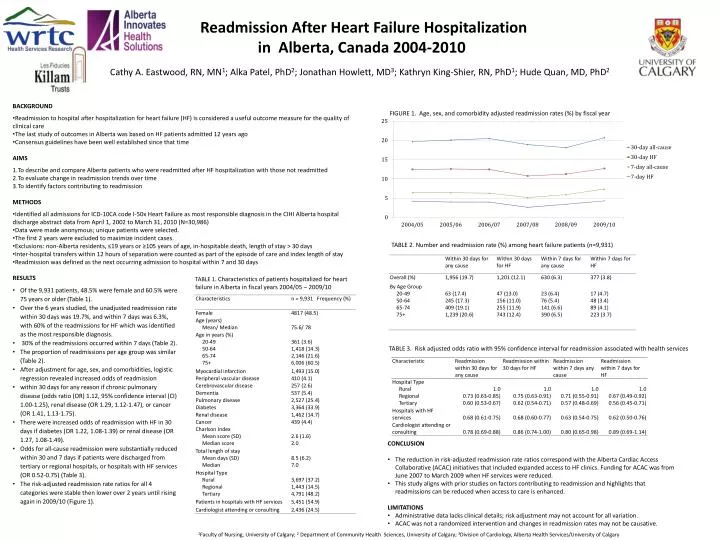
Readmission After Heart Failure Hospitalization in Alberta, Canada 2004-2010 Cathy A. Eastwood, RN, MN1; Alka Patel, PhD2; Jonathan Howlett, MD3; Kathryn King-Shier, RN, PhD1; HudeQuan, MD, PhD2 • BACKGROUND • Readmission to hospital after hospitalization for heart failure (HF) is considered a useful outcome measure for the quality of clinical care • The last study of outcomes in Alberta was based on HF patients admitted 12 years ago • Consensus guidelines have been well established since that time • AIMS • To describe and compare Alberta patients who were readmitted after HF hospitalization with those not readmitted • To evaluate change in readmission trends over time • To identify factors contributing to readmission • METHODS • Identified all admissions for ICD-10CA code I-50x Heart Failure as most responsible diagnosis in the CIHI Alberta hospital discharge abstract data from April 1, 2002 to March 31, 2010 (N=30,986) • Data were made anonymous; unique patients were selected. • The first 2 years were excluded to maximize incident cases. • Exclusions: non-Alberta residents, ≤19 years or ≥105 years of age, in-hospitable death, length of stay > 30 days • Inter-hospital transfers within 12 hours of separation were counted as part of the episode of care and index length of stay • Readmission was defined as the next occurring admission to hospital within 7 and 30 days FIGURE 1. Age, sex, and comorbidity adjusted readmission rates (%) by fiscal year TABLE 2. Number and readmission rate (%) among heart failure patients (n=9,931) • RESULTS • Of the 9,931 patients, 48.5% were female and 60.5% were 75 years or older (Table 1). • Over the 6 years studied, the unadjusted readmission rate within 30 days was 19.7%, and within 7 days was 6.3%, with 60% of the readmissions for HF which was identified as the most responsible diagnosis. • 30% of the readmissions occurred within 7 days (Table 2). • The proportion of readmissions per age group was similar (Table 2). • After adjustment for age, sex, and comorbidities, logistic regression revealed increased odds of readmission • within 30 days for any reason if chronic pulmonary disease (odds ratio (OR) 1.12, 95% confidence interval (CI) 1.00-1.25), renal disease (OR 1.29, 1.12-1.47), or cancer (OR 1.41, 1.13-1.75). • There were increased odds of readmission with HF in 30 days if diabetes (OR 1.22, 1.08-1.39) or renal disease (OR 1.27, 1.08-1.49). • Odds for all-cause readmission were substantially reduced within 30 and 7 days if patients were discharged from tertiary or regional hospitals, or hospitals with HF services (OR 0.52-0.75) (Table 3). • The risk-adjusted readmission rate ratios for all 4 categories were stable then lower over 2 years until rising again in 2009/10 (Figure 1). TABLE 1. Characteristics of patients hospitalized for heart failure in Alberta in fiscal years 2004/05 – 2009/10 TABLE 3. Risk adjusted odds ratio with 95% confidence interval for readmission associated with health services • CONCLUSION • The reduction in risk-adjusted readmission rate ratios correspond with the Alberta Cardiac Access Collaborative (ACAC) initiatives that included expanded access to HF clinics. Funding for ACAC was from June 2007 to March 2009 when HF services were reduced. • This study aligns with prior studies on factors contributing to readmission and highlights that readmissions can be reduced when access to care is enhanced. • LIMITATIONS • Administrative data lacks clinical details; risk adjustment may not account for all variation. • ACAC was not a randomized intervention and changes in readmission rates may not be causative. 1Faculty of Nursing, University of Calgary; 2 Department of Community Health Sciences, University of Calgary; 3Division of Cardiology, Alberta Health Services/University of Calgary






















