Download
1 / 22
220 likes | 421 Views
Exenetide and beta cell responses. Kolterman OG et al J Clin Endocrinol Metab 2003. Exenetide reduces A1C. Exenetide reduces A1C. Exenetide and insulin glargine. Exenetide and insulin glargine. Exenetide and insulin glargine. Exenetide and insulin glargine.

E N D
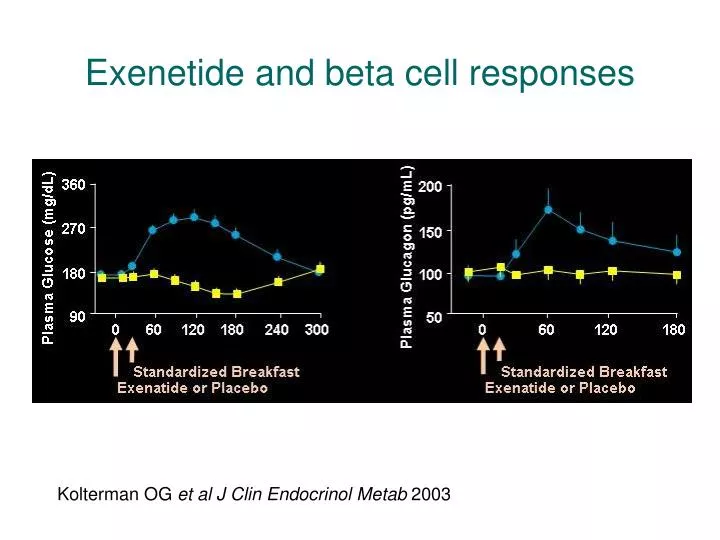
Exenetide and beta cell responses Kolterman OG et al J Clin Endocrinol Metab 2003
Exenetide and insulin glargine Heine et al. Annals Int Med 2005
Algorhythms for diabetes management • All agree: • lifestyle modification (diet, exercise, smoking cessation) • Reduce cardiometabolic risk (lipids, BP, ASA 325 mg) • metformin titrated to max tolerated dose • Intensify Rx if target A1C 6 to 7% • No agreement on next step: • SU e.g. glipizide XR • TZD e.g. pioglitazone, rosiglitazone • incretin mimetics e.g. exenatide (others on the way) • DP4 inhibitors, e.g. sitagliptin (others on the way) • insulin (? Which one)
Most Patients on Diabetes Therapies Not Reaching A1C < 7% 100 27% 32% 80 15% % of Subjects > 9% 19% 60 A1C Value 8%–9% 20% 7%–8% 22% 40 < 7% 38% 20 27% 0 Oral Insulin +/- oral *NHANES III = Third National Health and Nutrition Examination Survey. Harris MI, et al. Diabetes Care. 1999;22:403–408.
Clinical inertia: failure to intensify treatment of a patient who is not at their evidence-based A1C goal
Progressive Decline of β-Cell Function in the UKPDS 100 80 60 -Cell Function (% ) 40 20 0 10 9 8 7 6 5 4 3 2 1 0 1 2 3 4 5 6 Years Adapted from UK Prospective Diabetes Study (UKPDS 16) Group. Diabetes. 1995;44:1249-1258.
4T (Treating to Target in Type 2 DM) Year 1 Comparison of threesingle insulin regimens, added to OADs* Years 2 and 3 If HbA1c >6.5%, stop sulfonylurea and add a second insulin formulation Add biphasic insulintwice a day Add prandial insulinat midday R 708T2DMon dual OAD Add prandial insulinthree times a day Add basal insulinbefore bed Add basal insulinonce (or twice) daily Add prandial insulin three times a day * Intensify to a combinationisulin regimen in year one if unacceptable hyperglycaemia N Engl J Med 2007; 357: 1716-30
Biphasic * * Prandial * * * * * * * <> Basal * * Injection Self-measured glucose * 4T (Treating to Target in Type 2 DM) N Engl J Med 2007; 357: 1716-30
Dosing example of patient with type 2 diabetes on intensive insulin • A 56-year-old man with long-standing DM2, CAD, s/p MI, and recent CABG • Blood sugars high in hospital, where he was started on analog premix insulin 10 units bid • Insulin dose titrated over phone and during office visits • Office visit 6 months after cardiac surgery
Dosing example (cont’d) • No longer on oral agents • Now taking aspart mix 70/30 18 units with breakfast and 24 units with supper • Blood sugars ranging from 52 mg/dL to 265 mg/dL • A1C was 7.1%
Dosing example (cont’d) • Patient had retired early and used to enjoy playing golf at least twice a week • On golf days, he would develop hypoglycemia around midday • At one golf outing, he held his morning insulin, but his fingerstick went up to over 300 mg/dL
Solution (cont’d) • Daily insulin requirement = 24 + 18 = 42 units • Start basal insulin: about 50% of total insulin requirement = 42 units/d ÷ 2 = 21 units • Use fast-acting analog only with meals when patient is going to eat; vary time of administration on golf days; meet with dietitian CDE; adjust dose according to CHO to be consumed CDE = certified diabetes educator; CHO = carbohydrates.
Solution (cont’d) • Typical insulin-to-carb ratios 1:3 to 1:20 • This patient 1:5 • 31 g cereal + 15 g apple • 46 g carbs / 5 = 9 units aspart • 4 months later, A1C 6.4%; enjoying golf; lost 3 pounds; no hypoglycemia
Amylin • Reported in 1987 • 37-amino acid peptide Amylin Insulin Unger RH, Foster DW. Williams Textbook of Endocrinology (8th edition) 1992; 1273-1275 Photographs reprinted with permission of Elsevier
Amylin Activates Specific Areas of the rat brain amylin 10-8 M amylin 10-8 M amylin 10-8 M AC187 10-6 M 16 12 Spikes/s 8 4 0 0 30 60 90 120 150 180 Time (min) Rowland, et al. Regul Pept 1997; 71:171-174 Photographs from Riediger T, et al. Am J Physiol Regul Integr Comp Physiol 2001; 281:R1833-R1843
* * * * * * * pramlintide and glucose fluctuations Baseline (Insulin Only) 6 Months (Insulin + 120 mcg SYMLIN) 220 200 180 Glucose (mg/dL) 160 140 120 bedtime pre-lunch pre-dinner post-lunch pre-breakfast post-breakfast post-dinner n = 166 at baseline; observed cases; Mean (SE); *P-values for all data points <0.05 Data on file, Amylin Pharmaceuticals, Inc. See safety information with Boxed Warning in this presentation and the accompanying Prescribing Information



![Perreault S, et al. Eur J Clin Pharmacol 2009 Jun 16 [Epub]](https://cdn2.slideserve.com/3911021/slide1-dt.jpg)