Download
1 / 32
320 likes | 324 Views
Burkitt -like l ymphoma (probably diffuse blastoid B-cell lymphoma). Harleen K. Sidhu MD 1 Jagmohan S. Sidhu MD 2. Department of Dermatopathology, ClearPath Diagnostics, Syracuse, NY, USA Department of Pathology and Laboratory Medicine, UHS Hospitals, Johnson City, NY, USA.

E N D
Burkitt-like lymphoma(probably diffuse blastoid B-cell lymphoma) Harleen K. Sidhu MD1 Jagmohan S. Sidhu MD2 • Department of Dermatopathology, ClearPath Diagnostics, Syracuse, NY, USA • Department of Pathology and Laboratory Medicine, UHS Hospitals, Johnson City, NY, USA
Clinical Data • 74-year-old Caucasian male presented in March 2013 with a 4-month history of skin lesions on multiple sites of his body. • No fever, chills, night sweats, or weight loss. • Biopsy of a left flank skin lesion was performed.
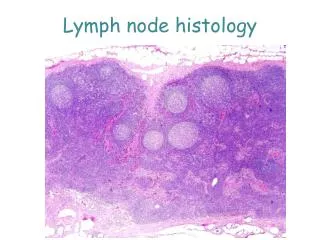
H&E X100 H&E X400
CD10 X400 CD20 X400
BCL2 X400 BCL6 X400 MUM1 X400 Ki67 X400
Other Negative Stains • CD2 • CD3 • CD4 • CD5 • CD7 • CD8
Diagnosis • Malignant lymphoma with features intermediate between diffuse large B-cell lymphoma and Burkitt lymphoma (Burkitt-like lymphoma) • The possibility of this lymphoma being a diffuse blastoid B-cell lymphoma [probably a histologically aggressive variant of t(14;18)-negative diffuse follicular lymphoma] was raised after a jejunal mass, which was detected in this patient by PET/CT, was worked-up more extensively.
F18-FDG PET/CT Scan • Increased uptake in the multiple nodular areas of skin and subcutaneous tissue and in 3 small bowel sites • Range of maximum SUV in skin/subcutis: 10-16.8 • Range of maximum SUV in small bowel: 10.5-17.2 • Maximum SUV (17.2) in the small bowel is in jejunum and is associated with 1 cm of small bowel wall thickening.
Surgical Resection and Gross Description • About 5.5 cm long segment of jejunum was resected to avoid possible perforation during chemotherapy. • A 5.5 cm small bowel segment with attached mesenteric tissue was received fresh. A 5 cm x 2 cm x 2cm “fish-flesh” like tumor was infiltrating the wall, protruding into the lumen and infiltrating the mesenteric tissue. Multiple small lymph nodes (0.3 cm -1.0 cm) were found in the mesentery. • Touch imprints of the jejunal mass were made and a piece of tumor was submitted for flow cytometric analysis. Rest of the specimen was fixed in 10% neutral buffered formalin.
Touch Imprint of Jejunal Mass DiffQuik Stain X1000
Scan of the Slides of Jejunal Mass CD20 BCL2 CD10 BCL6 MUM1 CD43 CD57 Ki67 HGAL LMO2 c-MYC p53 CD21 CD23 TdT BCL1 CD2 CD3 CD4 CD5 CD7 CD8 10 Recuts and 15 Unstained Sections of this block and 10 Recuts and 15 Unstained Sections of a skin block were submitted to the lymphoma workshop panel.
H&E Stain X200 H&E Stain X400
CD20 X400 CD10 X400
BCL2 X400 BCL6 X400 LMO2 X400 HGAL X400
MUM1 X400 CD57 X400
CD43 X400 Ki67 X400 MYC X400
Other Negative Stains • CD2 • CD3 • CD4 • CD5 • CD7 • CD8 • CD21 • CD23 • P53 • BCL1 • TdT
Flow Cytometric Analysis of Jejunal Mass • CD19+, CD20+, CD22+ (dim), CD38+, CD43+, CD57+, surface kappa+, • CD5-, CD10-, CD23-, CD79b-, CD200-, FMC7-, CD11c-, CD16-, CD56-
FISH of Jejunal MassDual Fusion Probes Dual-Color Dual Fusion Probe Tri-Color Dual Fusion Probe Normal IgH-BCL2 IgH: Green BCL2: Orange IgH/MYC Translocation in 66.50% nuclei IgH: Green MYC: Orange CEP8: Aqua Abnormal IgH-BCL2 IgH: Green BCL2: Orange
FISH of Jejunal MassBCL6 Dual Color Break-apart Probe Normal BCL6 3` BCL6: Green 5` BCL6: Orange BCL6 Rearrangement (an overhanging 5` BCL6 DNA sequence in 77% nuclei) 3` BCL6: Green 5` BCL6: Orange
FISH of Jejunal MassDual Color Probes No deletion/ monosomy of chromosome 7 7D7S522, CEP7 (7q31 - 7p11.1-q11.1) 7p11.1-q11.1 : Green 7q31 : Orange No deletion/ monosomy of chromosome 13 D13S319, LAMP1/13q (13q14.3-13q34) 13q34 : Green 13q14.3 : Orange
HGAL and LMO2 on Previous Skin/Subcutis Specimen LMO2 X400 HGAL X400
Diagnosis • High grade B-cell lymphoma, Burkitt-like (most probably a diffuse blastoid B-cell Lymphoma)involving skin and small intestine
Differential Diagnosis of Aggressive Diffuse B-cell LymphomaMorphologic Features MORPHOLOGY Our case has features highlighted in the red. Morphologically our case is not a diffuse large B-cell lymphoma, but it can be any other entity in the differential. DBBCL: Diffuse blastoid B-cell lymphoma DLBCL: Diffuse large B-cell lymphoma BL: Burkitt lymphoma DLBCL-BL: Intermediate between DLBCL and BL DBMCL: Diffuse blastoid mantle cell lymphoma B-LBL: B-lymphoblastic lymphoma
Differential Diagnosis of Aggressive Diffuse B-cell LymphomaImmunophenotypic Features IMMUNOPHENOTYPE Our case has features highlighted in the red. Immunophenotypically our case is not a DLBCL, DBMCL or B-LBL, but it can be DBBCL, BL or DLBCL-BL.
Differential Diagnosis of Aggressive Diffuse B-cell LymphomaCytogenetic Features NK: Not known CYTOGENETIC FEATURES Our case shows absence of t(14;18), presence of MYC translocation and presence of BCL6 rearrangement and, therefore, it is not a classic Burkitt lymphoma, can be called a Burkitt-like lymphoma or a Burkitt lymphoma with atypical features and is probably a diffuse blastoid B-cell lymphoma (DBBCL) . Other entities in the differential diagnosis have already been excluded by morphology and immunophenotyping.
Why is Our Case Not a Classic Burkitt Lymphoma (BL)? • Our case has a CD10+/BCL2+/BCL6+/MUM1+/CD57+ immunophenotype by immunohistochemistry • When a Burkitt lymphoma shows BCL2 expression, it can be called Burkitt lymphoma only if it has IgH/MYC translocation without BCL2 translocation and without BCL 6 translocation. • Our case shows BCL6 rearrangement, IgH/MYC translocation and absence of BCL2 translocation by FISH and conventional cytogenetic analysis.
Why did we raise the posssibility of a Diffuse blastoid B-cell lymphoma (DBBCL)? • Because it does not fit in any other entity in the differential diagnosis of aggressive B-cell lymphoma. • Because it shows many features of diffuse blastoid B-cell lymphoma that has been recently described and suggested as a histologically aggressive variant of t(14;18)-negative diffuse follicular lymphoma*. *Chiu A et al. Mod Pathol 2009;22:1507-1517
Treatment and Follow-Up • R-CHOP was initiated with almost 90% resolution of skin lesions after 1 cycle. • Chemotherapy was completed without any major complications. • Follow-up visit in December 2013: No lesions and no symptoms; normal PET/CT scan
Interesting Feature of Our Case Our case has a CD20+/CD10+/BCL2+/BCL6+/MUM1+/CD57+ immunophenotype with almost 100% Ki67 labeling index, shows BCL6 rearrangement and IgH/MYC translocation and shows absence of BCL2 translocation by FISH and conventional cytogenetic analysis. These features are those of a Burkitt-like lymphoma (Burkitt Lymphoma with atypical features) and are suggestive of diffuse blastoid B-cell lymphoma that has been described and suggested as a histologically aggressive variant of t(14;18)-negative diffuse follicular lymphoma in the literature (Chiu A et al. Mod Pathol 2009;22:1507-1517).