Download
1 / 2
20 likes | 127 Views
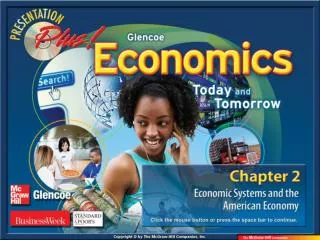
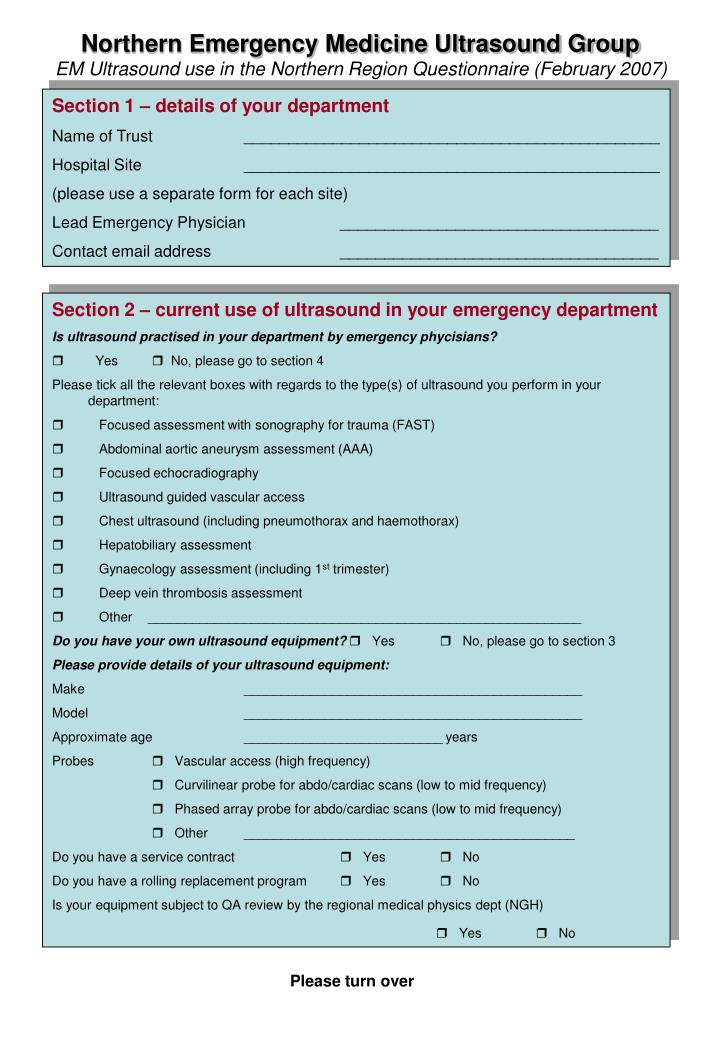
Northern Emergency Medicine Ultrasound Group EM Ultrasound use in the Northern Region Questionnaire (February 2007). Section 1 – details of your department Name of Trust _______________________________________________ Hospital Site _______________________________________________

E N D
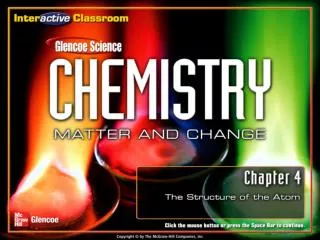
Northern Emergency Medicine Ultrasound GroupEM Ultrasound use in the Northern Region Questionnaire (February 2007) Section 1 – details of your department Name of Trust _______________________________________________ Hospital Site _______________________________________________ (please use a separate form for each site) Lead Emergency Physician ____________________________________ Contact email address ____________________________________ • Section 2 – current use of ultrasound in your emergency department • Is ultrasound practised in your department by emergency phycisians? • Yes No, please go to section 4 Please tick all the relevant boxes with regards to the type(s) of ultrasound you perform in your department: • Focused assessment with sonography for trauma (FAST) • Abdominal aortic aneurysm assessment (AAA) • Focused echocradiography • Ultrasound guided vascular access • Chest ultrasound (including pneumothorax and haemothorax) • Hepatobiliary assessment • Gynaecology assessment (including 1st trimester) • Deep vein thrombosis assessment • Other ___________________________________________________________ Do you have your own ultrasound equipment? Yes No, please go to section 3 Please provide details of your ultrasound equipment: Make ______________________________________________ Model ______________________________________________ Approximate age ___________________________ years Probes Vascular access (high frequency) Curvilinear probe for abdo/cardiac scans (low to mid frequency) Phased array probe for abdo/cardiac scans (low to mid frequency) Other _____________________________________________ Do you have a service contract Yes No Do you have a rolling replacement program Yes No Is your equipment subject to QA review by the regional medical physics dept (NGH) Yes No Please turn over
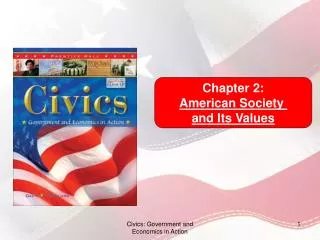
Section 3 – details of your emergency physicians performing ultrasound • Please list the names of members of staff including their training/experience level • Name _______________________________________________________ • Attended ultrasound introduction course – local/national (please circle) • Attended university short course/PgC/PgD/Masters (please circle) • Practices independently Approximate number of years performing ultrasound _________ years Approximate number of scans performed FAST ____ AAA ____ Lines ____ Other ____________ • Name _______________________________________________________ • Attended ultrasound introduction course – local/national (please circle) • Attended university short course/PgC/PgD/Masters (please circle) • Practices independently Approximate number of years performing ultrasound _________ years Approximate number of scans performed FAST ____ AAA ____ Lines ____ Other ____________ • Name _______________________________________________________ • Attended ultrasound introduction course – local/national (please circle) • Attended university short course/PgC/PgD/Masters (please circle) • Practices independently Approximate number of years performing ultrasound _________ years Approximate number of scans performed FAST ____ AAA ____ Lines ____ Other ____________ • Name _______________________________________________________ • Attended ultrasound introduction course – local/national (please circle) • Attended university short course/PgC/PgD/Masters (please circle) • Practices independently Approximate number of years performing ultrasound __________ years Approximate number of scans performed FAST ____ AAA ____ Lines ____ Other ____________ Please return this form to Bob Jarman, Consultant in Emergency Medicine, Queen Elizabeth Hospital, Gateshead, email bob.jarman@ghnt.nhs.uk • Section 4 – Interest in development of ultrasound in the Northern Region • Would you or any members of your staff be interested in the following: • Regional one day introduction to Emergency Medicine Ultrasound • Regional two day Level 1 – Theory and Introduction to Practice (with assessment) • Short Course in Emergency Ultrasound @ Teesside University (aimed at level 2 trainer) • Membership of Northern Emergency Medicine UltraSound group (NEMUS) • Guidance from NEMUS to help introduce ultrasound to your department • Become a dedicated training unit for level 1 training of Specialty Trainees