Download
1 / 31
330 likes | 535 Views
NEW MECHANISMS AND THERAPEUTIC TARGETS IN COPD. Peter Barnes FRS, FMedSci National Heart & Lung Institute Imperial College, London, UK. Turkish Thoracic Society: April 2014. Imperial College. Royal Brompton Hospital. What are the molecular mechanisms of amplification?

E N D
NEW MECHANISMS AND THERAPEUTIC TARGETS IN COPD Peter Barnes FRS, FMedSci National Heart & Lung Institute Imperial College, London, UK Turkish Thoracic Society: April 2014 Imperial College Royal Brompton Hospital
What are the molecular mechanisms of amplification? What are the genetic/epigenetic mechanisms? Mild COPD Severe COPD Exacerbation AMPLIFICATION OF INFLAMMATION IN COPD ++++ +++ Neutrophils Macrophages Cytokines Mediators Proteases Inflammation ++ + 0 Non-smokers Normal smokers
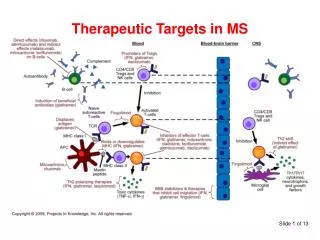
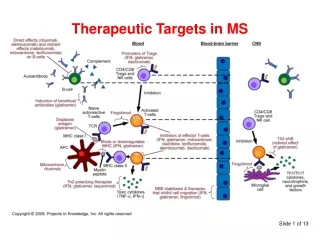
CXCL9 CXCL10 CXCL11 TGF-β CTGF CCL2 IL-23 CXCL1 CXCL8 Fibroblast CCR2 CXCR3 CXCR2 Th1 Tc1 Th17 Monocyte Tc1 Neutrophil Neutrophil elastase MMP-9 PROTEASES Fibrosis (Small airways) Alveolar wall destruction Mucus hypersecretion (Emphysema) INFLAMMATION IN COPD Barnes PJ: JCI 2008 Cigarette smoke (and other irritants) Epithelialcells Macrophage COPD inflammation is corticosteroid-resistant (in contrast to asthma) WHY?
Histone acetylation Inflammatory genes e.g. IL-8, MMP-9 Inflammation AMPLIFICATION AND STEROID RESISTANCE Corticosteroids Cigarette smoke Oxidative stress Glucocorticoid receptor NF-κB HDAC2
Peripheral lung HDAC2 Steroid resistance 3 2 HDAC2 expression (ratio vs histone-1) 1 *** ↑ Inflammation 0 Normal smokers COPD Non- smokers Ito K et al: N Engl J Med 2005 AMPLIFICATION AND STEROID RESISTANCE Cigarette smoke Oxidative stress NF-κB Histone acetylation HDAC2 Inflammatory genes e.g. IL-8, MMP-9
400 COPD macrophages 20000 Exhaled Peroxynitrite ** p<0.001 300 15000 Peroxynitrite (nM) HDAC activity (AFU/10µg) 200 10000 ↑PI3Kδ P 5000 Akt 100 Ub Ub NO Tyr Ub 0 Ub Ub P Ub B/L Theophylline (10-6M) Ub Ub ↓HDAC2 ↓HDAC2 ↓HDAC2 0 Cosio B et al: J Exp Med 20 04 NCOPD Osoata G et al: Chest 2009 CORTICOSTEROID RESISTANCE IN COPD Oxidative stress Nitrative stress Peroxynitrite HDAC Cell membrane ↓HDAC2 Steroid resistance
Antioxidants Nrf2 activators ↓ PI3Kδ THEOPHYLLINE Nortriptyline ↓ Akt-1 Macrolides PI3Kδ inhibitors ↑HDAC2 Akt inhibitors GSK3β activators Reversal of steroid resistance HDAC2 activators? REVERSAL OF CORTICOSTEROID RESISTANCE Oxidative stress Cell membrane ↑PI3Kδ P Akt P ↓HDAC2 Steroid resistance
OXIDATIVE STRESS Ub Antioxidants mRNA Nrf2 AND ANTIOXIDANT GENE REGULATION BZip transcription factor Nrf2(-/-): ↑ emphysema in smoking mice Rangasamy T et al: :JCI 2004; Ishii et al: J Immunol 2005 Nrf2 Keap-1 Nrf2 activity in lung ↑ in normal smokers ↓ in COPD patients Malhotra D et al: AJRCCM 2008 No ↑ with ox stress in COPD Due to Nrf2 acetylation from ↓ HDAC2 Mercado N et al: BBRC 2010 Nucleus ARE Antioxidant genes (GPX, HO-1, catalase etc)
Nrf2 acetylation 2.0 * 1.5 1.0 Acetylated:total Nrf2 0.5 0.0 C TSA Nrf2 REGULATION IN COPD Nrf2-ARE binding 0.50 * ** Oxidative stress Lung +H2O2 Relative adsorbance 0.25 ↓HDAC2 Ac Nrf2 0 COPD Healthy Smoker ARE gene transcription ↓Antioxidants ↑Oxidative stress Mercado N et al: BBRC 2011
HDAC2 activity (COPD macrophages) 10 ** 8 Sulforaphane (isothiocyanate) Destabilises KEAP-1→↑Nrf2 6 HDAC2 (μM/μg protein) 4 2 0 Contr Sulfo HDAC activity in vivo 30 ** Mice Nrf2+/+ HDAC activity (μM/μg protein) 20 Nrf2-/- Broccoli Broccoli sprouts Wasabi 10 Malhotra D et al: J Clin Invest 2011 0 Contr Sulfo SULFORAPHANE ↑ HDAC2 VIA Nrf2 ACTIVATION • Nrf2 activators as therapeutics • Sulforaphane: clinical trial in COPD • Triterpenoids: bardoxelone methyl (CDDO) • high toxicity • Olipraz (dithiolethione) • Dimethyl fumarate (BG12): now approved in MS • Novel Nrf2 activators
High risk of side effects Inhaled delivery needed IMPLICATIONS FOR NEW TREATMENTS • New anti-inflammatory treatments • PDE4 inhibitors • p38 MAP kinase inhibitors • IKK-2 (NF-κB) inhibitors • pan-JAKinhibitors • Alternative approach: Restore steroid sensitivity! • Repurposing existing therapies: • Low dose oral theophylline • Oral nortriptyline, macrolides • Development of new therapies: • Inhaled PI3Kδ, PI3Kγ/δ inhibitors (RespiVert/J&J) • Non-antibiotic macrolides • Theophylline is cheap, safe in low doses, oral (small airways) • suitable for oral combinations • Long-term controlled trials (1 yr) with theophylline in COPD • Low dose oral theophylline (plasma conc ~5mg/L) • + low dose inhaled steroid: UK NHS study (TWICS) • Low dose oral theophylline • + low dose oral steroid (prednisone 5mg): China (TASCS)
Antioxidants Oxidative stress COPD Anti-ageing molecules? Geroprotectors ACCELERATED AGEING IN COPD Normal ageing 100 50 0 Senile emphysema Lung function (% max) 25 60-70 80-90 160 Age (yr) Ito K, Barnes PJ: Chest 2009
Oxidative stress UV irradiation Telomere shortening Replicative senescence DNA damage AGEING PROGRAMMED NON-PROGRAMMED Counteracted by anti-ageing molecules including: sirtuins SIRT1, SIRT6 HDAC2 FOXO3a Nrf2 Klotho, SMP30
0.2 SIRT1 protein r=0.658 p<0.001 6 p<0.001 SIRT1/GNB2L1 0.1 4 SIRT1/lamine A/C 0.0 0 25 50 75 100 2 FEV1/FVC (%) Good correlation with FEV1 (r=0.72) 0 smoker COPD non-smoker Nakamuru Y et al: FASEB J 2009 ↓ SIRT1 IN COPD Sirtuin SIRT1: anti-ageing and repair molecule protein deacetylase (non-histone proteins) ↓ SIRT1 expression in COPD lung and PBMC Also ↓SIRT6; SIRT2,3,4,5,7 normal
SIRT1 mRNA SIRT1 lamin 0 4 24 h H2O2 (200μM) OXIDATIVE STRESS ↓ SIRT1 U937 cells 4000 SIRT1 activity 3000 AFU ** 2000 1000 0 H2O2 (200μM) Cntrl Nakamuru Y et al: FASEB J 2009
SIRT1 siRNA * 5 MMP-9 mRNA 4 3 MMP-9/GAPDH mRNA 2 1 0 * MMP-9 activity 1.5 1.0 Activity-OD 0.5 0 B/L PMA Scr SIRT1- ↓ SIRT1 ↑MMP9 U937 cells SIRT inhibitor * 15 MMP-9 mRNA 10 MMP-9 mRNA (% GAPDH) 5 0 * 1.5 MMP-9 activity 1.0 Activity-OD 0.5 0 B/L PMA PMA + Splitomycin (100 μM) Nakamuru Y et al: FASEB J 20099
↑ Oxidative stress ↑ Oxidative stress Ac Ac Ac Ac Ac ↓Ku70 ↑ p53 ↓FoxO3a ↑NF-κB ↓Nrf2 ↑ MMP-9 ↑ IL-8 ↓ DNA Repair ↑ Inflammation ↑ Aging EFFECTS OF ↓ SIRT1 ↓SIRT1
RESTORING SIRT1 Antioxidants Nrf2 activators Theophylline Nortriptyline PI3Kδ inhibitors AMPK Metformin Rapamycin Sirtuin activators Resveratrol Oxidative stress Cell membrane ↑PI3Kδ ↑Akt ↑ mTOR ↓SIRT1 ↑ LUNG AGEING
Zymography PMA PMA+RV MMP-9 120 • SIRTUIN ACTIVATORS (STACs) • Plant polyphenols: • Resveratrol • Quercitin • Piceatannol • Poor oral bioavailability • More potent synthetic SIRT1 activators (e.g. SRT2172) • Inhaled resveratrol? MMP-9 activity 100 80 IC50=9μM MMP-9 (% control) 60 40 20 0 0.1 1 10 100 Resveratrol (μM) RESVERATROL ON SIRT1 AND MMP-9 U937 cells SIRT1 activity 1000 10x↑ SIRT1 activity (% basal) 500 0 0 1 10 100 Resveratrol (μM)
MMP-9 activity U937 cells exposed to H2O2 120 280 100 Resveratrol SRT-2172 (Sirtris) 240 80 SRT-2172 200 % of control 60 % Activation 160 40 120 20 80 0 4 0 9 6 8 5 7 9 8 6 7 5 Concentration (-log,M) Concentration (-log,M) SIRT ACTIVATOR SIRT1 activation Nakamuru Y et al: FASEB J 2009
** ** ** SRT Dex SIRT ACTIVATOR IN SMOKING MICE SRT-2171 MMP-9 expression SIRT1 activity ** ** ** ** 20 5 4 15 MMP-9/GAPDH 3 SIRT1 activity (unit/ug protein) 10 2 5 1 0 0 Sal Sal SRT Dex Sal Sal Air Air Smoke Smoke Nakamuru Y et al: FASEB J 2009
↓ SIRT1 AND ACCELERATED AGING ↑ LUNG AGING Increased skin-wrinkling In COPD patients Patel BD et al: Thorax 2006 Diabetes Metabolic syndrome Osteoporosis Emphysema Skin wrinkling Skin wrinkling associated with ↑ dermal MMP-9 ↓eNOS ↑MMP9 ↓LV function ↑ Arterial stiffness Atherosclerosis Hypertension Cardiac failure ↑ CARDIOVASCULAR AGING Oxidative stress ↑PI3Kδ ↓SIRT1
ECFC 3 2 Cell number/well x 103 Matrigel VWF+/CD45- 1 0 Normal COPD ENDOTHELIAL PROGENITOR CELLS Endothelial colony forming cells 7-22 days • COPD vs controls • Proliferation +/- VEGF: unchanged • Migration: unchanged • ↓ Angiogenesis • ↑ Apoptosis • Failure to repair endothelial injury Paschalaki K et al: Stem Cells 2013
Senescence-associated β-galactosidase 0.3 P<0.01 EPCSIRT1 activity 200 0.2 SA-β-GAL + /total cells P<0.05 SIRT1 activity (OD/μg protein) 100 0.1 0 Normal COPD 0 Normal COPD (n=9) (n=11) Correlated with ↑ SA-β-GAL ↑ CELLULAR SENESCENCE IN EPC FROM COPD Normal (72yr) EPCeNOS * eNOS protein COPD (69 yr) Normal COPD SA-β-GAL Paschalaki K et al: Stem Cells 2013
Cigarettesmoke Wood smoke ROS HDAC Steroid response NO Phagocytosis LTB4 CXCL1 CXCL8 Elastolysis MMP-9, MMP-12 Cathepsins B,L,K CCL2 CXCL1 CXCL9 CXCL10 CXCL11 CXCR2 CCR2 CXCR2 CXCR3 Emphysema Neutrophils Monocytes CD8+ cells ALVEOLAR MACROPHAGES IN COPD • Numbers (25X) • ↑ Mediator secretion • Steroid resistance • “M2-like” Chana K et al: JACI 2013
MDM +10% FCS +GM-CSF x 12d 6 6 ns 4 4 * * Phagocytosed E coli (μg) ns 2 ns 2 0 Non-sm Sm COPD 0 COPD Sm COPD Non-sm ↓ MACROPHAGE PHAGOCYTOSIS IN COPD Alveolar Macrophages Monocytes Fluorescent E coli uptake 6 ns 4 Phagocytosed E coli (μg) Phagocytosed E coli (μg) 2 0 Sm Non-sm Taylor AE et al: Eur Resp J 2010
0.10 Strep. pneumoniae 0.08 0.06 Phagocytosis 0.04 ** 0.02 0.00 Normal Smoker COPD ↓ MACROPHAGE PHAGOCYTOSIS IN COPD Monocyte-derived macrophages Haemophilusinfluenzae 0.05 ↓Phagocytosis of bacteria (Gram +ve and -ve) Normal phagocytosis of inert beads Abnormality in scavenger receptors? 0.04 0.03 Phagocytosis 0.02 ** 0.01 0 Normal Smoker COPD Taylor AE et al: Eur Resp J 2010
COPD Defective phagocytosis ↑ Inflammatory mediators Chronic colonisation Persistent inflammation MACROPHAGE PHAGOCYTOSIS • Non-smoker • Normal smoker Alveolar macrophage Scavenger receptors MARCO, CD36, CD163, Mannose receptor, PS receptor Bacteria Apoptotic neutrophils Sterilisation of Respiratory tract Resolution of inflammation
Strep. pneumoniae 15 * 10 RFU (x103) 5 0 ≥3 exac/y ≤1 exac/yr Infrequent Frequent FREQUENT vs INFREQUENT EXACERBATORS Bacterial phagocytosis by MDMs H. influenzae 20 ** • New treatments to restore bacterial phagocytosis • Microtubular stabilisers (epothilone) • New signalling pathways identified (e.g. S1P pathway) 15 RFU (x103) 10 5 0 ≥3 exac/y ≤1 exac/yr Infrequent Frequent Catherine Thomas
CONCLUSIONS • Corticosteroid resistance in COPD • - via oxidative stress: ↓HDAC2, ↑PI3Kδ • - reversed by theophylline, macrolides, PI3Kδ inhibitors, • Nrf2 activators • Accelerated aging in COPD: cellular senescence • Anti-aging molecules: SRT activators, PI3K inhibs, metformin • New approaches include restoring defective phagocytosis • e.g. microtubular stabilisers • Understanding COPD mechanisms • Identifies new treatment targets • More effective therapy in the future to • ↓ disease progression, ↓ mortality • ↓ exacerbatons, ↓ comorbidities
ACKNOWLEDGEMENTS Ian Adcock Kylie Belchamber BorjaCosio Gaetano Caramori Kiran Chana Fan Chung Louise Donnelly Paul Ford Kaz Ito Ellen Jazrawi Masa Kagoshima Yoshi Kobayashi John Marwick Nico Mercado Grace Osoata Koralia Paschalaki Anna Randi Richa Singh Abigail Taylor Catherine Thomas Yasuo To Wisia Wedzicha Jim Hogg (Vancouver, Canada) Yasuo Kizawa (Tokyo, Japan) ShyamBiswal (Baltimore, USA) Sundeep Salvi (Pune, India) NHLI Imperial College FUNDED BY: Wellcome Trust MRC AstraZeneca Cempra GSK Mitsubishi-Tanabe Novartis Pfizer Royal Brompton Hospital