Download
1 / 21
210 likes | 212 Views
This presentation discusses the importance of implementing newborn hearing screening in homebirth settings and the role of midwives in providing this service. It covers the challenges, objectives, and steps taken to establish a partnership between state EHDI offices and midwives. The training guide created for midwives is also shared, along with future plans for expanding the program.

E N D
Newborn Hearing Screening in Homebirth Settings: The Midwife’s Role URLEND Trainees Nancy Pajak (Wyoming) Becky Larsen (Utah) Nancy Dold (Montana) Presentation Date – April 30, 2010
In the Beginning… • Problem: Newborn Hearing Screening (NHS) is not provided for all newborns • How do we reach those babies who are born outside the hospital setting? • Community health fairs, local clinics, midwives???
Community Health Fair • Advantage: Provide access to a larger population at one event • Challenges: Initial plan takes time in identifying stakeholders and establishing partnerships • As a leadership project, IRB approval may be necessary
Narrowing the Scope • “Even if we just identify one individual who needs hearing intervention, then we are making progress” • Reaching out to homebirth populations • Establishing a partnership with the midwife
The Leadership Project • Rationale: • The average rate of infants screened for the states within the URLEND region is 96.7% (CDC, 2007) • a sharp increase of births attended by midwives, either in the home or in a birthing center, from 1975 -2006(National Vital Statistics Report, 2009) • Families who choose a homebirth environment will not have access to newborn hearing screening unless provided through the midwife attending the birth. • The State EHDI office will serve as a resource for education, training and equipment for the midwifery system.
Project Objectives • Develop a system of NHS service through education, training and providing equipment resources to midwives • Expand the number of newborn hearing screenings to families that choose homebirth environments • Provide hearing screenings within the home through the midwife to other children who may have not been screened • Identify children with hearing loss among the homebirth population • Create a working partnership between state EDHI offices and midwives within the state • Educate midwives and families in the importance of newborn hearing screening and early intervention for children with hearing loss • Foster and encourage hearing health for all members of the family
First Step • Establishing a relationship with the midwife – midwives were identified in the Wyoming area for the purpose of the project • Establishing trust and creating a partnership • Developing a partnership network
Education and Training • Identified sources for educational and training materials – Literature review, National Center on Hearing Assessment and Management, Medical Home, and Utah EHDI training manual • Compiled a training guide: Newborn Hearing Screening: A Guide for the Midwife
A Guide for the Midwife • General Information • Newborn Hearing Screening Protocol • Diagnostic Follow-up and Early Intervention Resources • Frequently Asked Questions • References and Recommended Reading
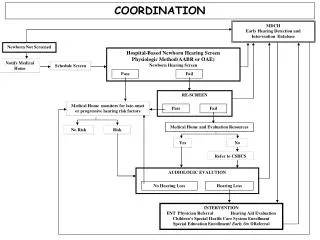
Hearing Screening Protcol • First screening 24 hours after birth • If needed, the infant will be re-screened • After the second screening, if the infant does not pass, the infant will be referred for a complete audiometric evaluation • Contact information for facilities with complete evaluations is available for parents • Parents who choose not to have their infant’s hearing screened are required to sign a waiver form
Midwife Training at Walcott Junction, Wyoming • One midwife to do hearing screening after home births • Hearing screenings will be done 24 hours after birth • Otoacoustic Emission (OAE) equipment from the state EDHI program will be available for the midwife to use
Suggestions from the Midwife • While the training manual was helpful, the midwife suggested changing some terminology to reflect a home birth model as opposed to a medical model. • For instance, the midwife believed that the terminology ‘refer’ indicated that the newborn should be referred immediately to the physician. • The midwife suggested using the term ‘fail’ instead. While there are problems with the implications of the use of ‘fail’, especially for the parents, the midwife does have a good point here.
A Fortuitous Event Later, on the same day of midwife training, a prospective client asked the midwife whether or not hearing screening was part of the package of services The midwife was delighted to be able to say that hearing screening was indeed a part of the services offered
Further… The trained midwife gave the Wyoming EHDI program hearing screening training for midwives a favorable review! She will encourage other midwives in Wyoming to train in newborn hearing screening
Future Plans • Practicing with the OAE equipment will continue in June • The midwife will report… • numbers of children screened • recommended follow-up actions to the Wyoming EHDI program • names of children screened (with parental consent)
Reflections on the URLEND Experience • Very valuable! • Attending clinics at Salt Lake City, Logan and Ogden • Attending Investing in Family Support conference in Scottsdale • Attending EHDI conference in Chicago • Meeting others with similar goals and aspirations and sharing ideas and plans
Reflections on Leadership Growth • Our group agreed that leadership growth was reflected in our collective journey through the Leadership Project • Appreciated most – the interpersonal connections that were made by the three of us • Three people – three different States (Wyoming, Utah & Montana) – have made connections for life and we know we could call on each other at any point in time for advice or help
Reflections on Future Leadership Activities • Future leadership activities really depend on the overall goal of URLEND and the participant interests • Suggestion – perhaps five previous Leadership Projects should be selected as reading assignments at the beginning of the URLEND year
Feedback on URLEND Program • The URLEND program is not for the faint-hearted! • This is a rigorous program with weekly readings and assignments as well as projects • Diverse group with various learning styles and experience • Suggestions: • A module on conducting research (The great and powerful IRB) • A trainee mentor • A list of readings and assignments before the first seminar
Feedback on Development of Leadership Skills under URLEND • Greater awareness was gained… • Hearing loss (etiology, prevention & amelioration, current trends) • Autism (current issues along with the changing inclusion criteria) • The Family (issues in raising kids with special healthcare needs) • Greater awareness will continue to inform future action and involvement