Download
1 / 67
670 likes | 677 Views
Infection and Defects in Mechanisms of Defense. Chapter 7. Microorganism and Human Relationship. Mutual relationship Normal flora Relationship can be breached by injury Leave their normal sites and cause infection elsewhere Opportunistic microorganisms. Factors for Infection.

E N D
Microorganism and Human Relationship Mutual relationship Normal flora Relationship can be breached by injury Leave their normal sites and cause infection elsewhere Opportunistic microorganisms
Factors for Infection Communicability Ability to spread from one individual to others and cause disease: measles and pertussis spread very easily, HIV is of lower communicability Immunogenicity Ability of pathogens to induce an immune response
Factors for Infection (cont’d) Infectivity Ability of pathogen to invade and multiply in the host Involves attachment to cell surface, release of enzymes, escape phagocytes, spread through lymph and blood to tissues Pathogenicity Ability of an agent to produce disease Success depends on communicability, infectivity, extent of tissue damage, and virulence
Factors for Infection (cont’d) Mechanism of action How the microorganism damages tissue Portal of entry Route by which a pathogenic microorganism infects the host Direct contact Inhalation Ingestion Bites of an animal or insect
Factors for Infection (cont’d) Toxigenicity Ability to produce soluble toxins or endotoxins, factors that greatly influence the pathogen’s degree of virulence Virulence Capacity of a pathogen to cause severe disease; for example, measles virus is of low virulence; while rabies virus is highly virulent
Classes of Infectious Microorganisms Virus Bacteria Fungi Protozoa Chlamydia Rickettsia Mycoplasma Helminths
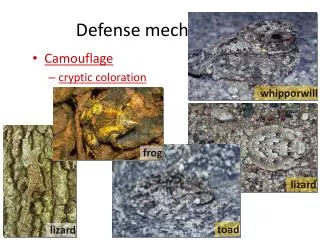
Pathogen Defense Mechanisms Bacteria Produce surface coats that inhibit phagocytosis and toxins Viruses Many can mutate within cells where they are not available to immune and inflammatory mechanisms Not available to antibodies in circulation Antigenic variations: Antigenic drift Antigenic shifts
Bacterial Virulence and Infectivity Toxin production Exotoxins (cytotoxins, neurotoxins, pneumotoxins, enterotoxins, hemolysins) Enzymes released during growth, causing specific responses Immunogenic Antitoxin production Endotoxins Lipopolysaccharides contained in the cell walls of gram-negative organisms released during cell destruction Pyrogenic effects
Bacterial Virulence and Infectivity (cont’d) Bacteremia (presence) or septicemia (growth) A result of a failure of the body’s defense mechanisms Usually caused by gram-negative bacteria Toxins released in the blood cause the release of vasoactive peptides and cytokines that produce widespread vasodilation leading to septic (endotoxic) shock
Viral Infection Characteristics: Dependent on host cells No metabolism Simple organism Spreads cell to cell Usually a self-limiting infection
Viral Replication Not capable of independent reproduction Need permissive host cell Begins when virion binds to a specific receptor on the plasma membrane of a host cell penetrates the plasma membrane Virus then uncoats in cytoplasm DNA virus replicates in nucleus RNA virus replicates in cytoplasm
Viral Replication (cont’d) Copies of genetic material made New virions released from cell to infect other host cells Some remain latent in host cell until activated by stress, hormone changes, disease (e.g., herpes virus and cold sore)
Cellular Effects of Viruses Inhibition of host cell DNA, RNA, or protein synthesis Disruption of lysosomal membranes release enzymes that damage host cell Transformation of host cell to cancer cell Promotion of secondary bacterial infection
Cellular Effects of Viruses (cont’d) Fusion of infected, adjacent host cells to produce giant cells Alteration of antigenic properties of host cell leading to immune system attack of cell as foreign
Fungal Infection Large microorganisms with thick rigid cell walls without peptidoglycans (resist penicillin and cephalosporins) Eukaryotes Exist as single-celled yeasts, multi-celled molds, or both Reproduce by simple division or budding
Fungal Infection (cont’d) Pathogenicity Adapt to host environment Wide temperature variations, digest keratin, low oxygen Suppress the immune defenses Usually controlled by phagocytes, T lymphocytes
Fungal Infection (cont’d) Diseases caused by fungi are called mycoses Superficial, deep, or opportunistic Fungi that invade the skin, hair, or nails are known as dermatophytes The diseases they produce are called tineas (ringworm) Tinea capitis, tinea pedis, and tinea cruris
Fungal Infection and Injury Deep fungal infections are life threatening and are commonly opportunistic (e.g., with antibiotics or pH changes) Changes that alter normal flora foster fungal infections
Parasitic Infection Symbiotic Unicellular protozoa to large worms (helminths) Flukes, nematodes, tapeworms Protozoa include malaria, amoebae, flagellates More common in developing countries Spread human to human via vectors Usually ingested Tissue damage is secondary to infestation itself with toxin damage or from inflammatory/immune response
Clinical Manifestations of Infectious Disease Variable depending on the pathogen Directly caused by the pathogen or indirectly caused by its products Fever Beneficial Resetting the hypothalamus Exogenous pyrogens from organisms produce endogenous pyrogens Endogenous pyrogens (cytokines) including interleukins
Countermeasures Vaccines Induction of long-lasting protective immune responses that will not result in disease in a healthy recipient Attenuated organism Killed organisms Recombinant viral protein Bacterial antigens Toxins
Countermeasures (cont’d) Antimicrobials Bacteriocidal vs. bacteriostatic Inhibit synthesis of cell wall Damage cytoplasmic membrane Alter metabolism of nucleic acid Inhibit protein synthesis Modify energy metabolism
Countermeasures (cont’d) Antimicrobial resistance Genetic mutations Inactivation Multiple antibiotic-resistance bacteria (e.g., MRSA) Can destroy normal flora C difficile
Countermeasures (cont’d) Vaccines Biologic preparations of weakened or dead pathogens Long lasting immunity CDCP schedules Development expensive Reluctance to vaccinate but complications rare
Immune Deficiencies Failure of immune mechanisms of self-defense Primary (congenital) immunodeficiency Genetic anomaly Secondary (acquired) immunodeficiency Caused by another illness More common
Immune Deficiencies (cont’d) Clinical presentation Development of unusual or recurrent, severe infections T cell deficiencies Viral, fungal, yeast, and atypical microorganisms B cell and phagocyte deficiencies Microorganisms requiring opsonization Complement deficiencies
Primary Immune Deficiencies Most are the result of a single gene defect Five groups: B lymphocyte deficiencies T lymphocyte deficiencies Combined T and B cell deficiencies Complement defects Phagocyte defects
B Lymphocyte Deficiencies Hypogammaglobulinemia or agammaglobulinemia Bruton agammaglobulinemia Autosomal agammaglobulinemia X-linked hyper-IgM syndrome IgG subclass deficiency Selective IgA deficiency Common variable immune deficiency
T Lymphocyte Deficiencies DiGeorge syndrome Partial or complete absence of T cell immunity Chronic mucocutaneous candidiasis
Combined T and B Cell Deficiencies Severe combined immunodeficiency (SCID) Reticular dysgenesis (most severe form) Adenosine deaminase (ADA) deficiency X-linked SCID JAK3 deficiency IL-7 receptor deficiency Purine nucleoside phosphorylase deficiency
Combined T and B Cell Deficiencies (cont’d) RAG-1 or RAG-2 deficiency Bare lymphocyte deficiency MHC class I and II deficiency Wiskott-Aldrich syndrome Ataxia-telangiectasia (AT)
Complement Deficiencies C3 deficiency Mannose-binding lectin (MBL) deficiency Properdin deficiency Factor I and factor H deficiency C9 deficiency
Phagocytic Deficiencies Severe congenital neutropenia Cyclic neutropenia Leukocyte adhesion deficiencies (LAD) C3 receptor deficiency Chédiak-Higashi syndrome Myeloperoxidase deficiency Chronic granulomatous disease
Secondary Deficiencies Also referred to as acquired deficiencies Far more common than primary deficiencies Often not clinically relevant
Secondary Deficiencies (cont’d) Causes: Normal physiology conditions Psychologic stress Dietary insufficiencies Malignancies Physical trauma Medical treatments Infections Acquired immunodeficiency syndrome (AIDS)
Acquired Immunodeficiency Syndrome (AIDS) Syndrome caused by a viral disease Human immunodeficiency virus (HIV) Depletes the body’s Th cells Incidence: Worldwide: 33.4 million (2008) United States: about 56,000 (2008)
Acquired Immunodeficiency Syndrome (AIDS) (cont’d) Effective antiviral therapies have made AIDS a chronic disease Epidemiology Blood-borne pathogen Heterosexual activity is most common route worldwide Increasing faster in women than men especially in adolescents
Acquired Immunodeficiency Syndrome (AIDS) (cont’d) Pathogenesis Retrovirus Genetic information is in the form of RNA Contains reverse transcriptase to convert RNA into double-stranded DNA Integrase Protease
Human Immunodeficiency Virus (HIV) (cont’d) Structure gp120 protein binds to the CD4 molecule found primarily on surface of helper T cells Destroys CD4+ Th cells Typically 800 to 1000 cell/mm3 Reverses CD4/CD8 ratio
Human Immunodeficiency Virus (HIV) (cont’d) Clinical manifestations Serologically negative, serologically positive but asymptomatic, early stages of HIV, or AIDS Window period Th cells <200 cells/mm3 diagnostic for AIDS Diagnosis of AIDS is made in association with various clinical conditions and lab tests: Atypical or opportunistic infections, and cancer Presence of antibodies against HIV (4 to 7 weeks after blood transmission, 6-14 months after sexual intercourse) Western blot analysis
Human Immunodeficiency Virus (HIV) (cont’d) Treatment and prevention Highly active antiretroviral therapy (HAART) Reverse transcriptase inhibitors Protease inhibitors New drugs Entrance inhibitors Integrase inhibitors Vaccine development
Evaluation of Immunity Complete blood count (CBC) with a differential Subpopulations of lymphocytes Quantitative determination of immunoglobulins Subpopulations of immunoglobulins Assay for total complement Skin tests
Treatment for Immunodeficiencies Gamma-globulin therapy Stem cell transplantation Transfusion of erythrocytes Treatment with soluble immune mediators Gene therapy Caution with immunizations
Hypersensitivity Altered immunologic response to an antigen that results in disease or damage to the host
Hypersensitivity (cont’d) Allergy Deleterious effects of hypersensitivity to environmental (exogenous) antigens Autoimmunity Disturbance in the immunologic tolerance of self-antigens Alloimmunity Immune reaction to tissues of another individual
Hypersensitivity (cont’d) Characterized by the immune mechanism: Type I IgE mediated Type II Tissue-specific reactions Type III Immune complex mediated Type IV Cell mediated
Hypersensitivity (cont’d) Immediate hypersensitivity reactions Anaphylaxis Delayed hypersensitivity reactions
Type I Hypersensitivity IgE mediated Against environmental antigens (allergens) IgE binds to Fc receptors on surface of mast cells (cytotropic antibody) - “sensitized” Histamine release H1 and H2 receptors Antihistamines