Download
1 / 31
310 likes | 524 Views
WINDSOR UNIVERSITY SCHOOL OF MEDICINE St.Kitts. Dr. SREEKANTH THOTA. DEPARTMENT OF ANATOMY. UPPER LIMB. Upper limb joints . Type Articulation Ligaments Movements Blood Supply Nerve Supply. Glenohumeral Joint. SHOULDER JOINT TYPE: Synovial : ball and socket joint Bony articulation

E N D
WINDSOR UNIVERSITYSCHOOL OF MEDICINESt.Kitts Dr. SREEKANTH THOTA DEPARTMENT OF ANATOMY UPPER LIMB Upper limb joints
Type • Articulation • Ligaments • Movements • Blood Supply • Nerve Supply
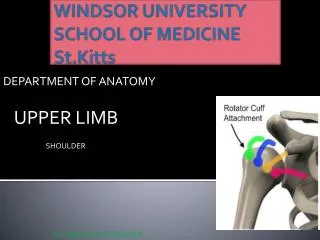
Glenohumeral Joint • SHOULDER JOINT • TYPE: • Synovial : ball and socket joint • Bony articulation • -Head of the Humerus • -Glenoid cavity of the Scapula • (deepened by Glenoid labrum)
Important Relation • Anteriorly • Subscapular, • Axillart vessels, BP • Posteriorly • Infraspinatus, TMin • Superiorly • Supraspinatus, • Subacromial Bursa • Coracoacromiallig., Deltoid m. • Inferiorly • Long head of Triceps, Axillary n • Post.circumflex humeral artery.
Bursa of Shoulder Joint Contain thin layer of synovial fluid Located where tendons rub against bone, ligaments, or tendons and when skin moves over bone directly beneath Subscapular bursa Subacromial (subdeltoid) bursa
Subscapular bursa • Between tendon of subscapularis muscle and neck of scapula • Communicates with cavity of shoulder joint • Subacromial (subdeltoid) bursa • Between deltoid, supraspinatus tendon and glenohumeral capsule • Does not communicate with cavity of shoulder • Facilitates movement of deltoid over joint capsule and supraspinatus tendon under coracoacromial arch
Movements: • Mobile but unstable joint • - The head of the humerus doesn’t fit perfectly with the glenoidfossa and Glenoid labrum
FLEXION • Pectoralis Major • Deltoid m.(anterior.fibres) • Bicpes • Coracobrachialis • EXTENSION • * LatissimusDorsi • * teres Major • * Triceps –long head
ABDUCTION • Deltoid m.(mid.fibres) • Supraspinatus m. • ADDUCTION • Pectoralis major, LatissimusDorsi, Teres Major • LATERAL ROTATION. • Infraspinatus, Teres minor • Deltoid (post. fibres) • MEDIAL ROTATION. • Subscapular, LatisimusDorsi • Deltoid (ant. fibres)
Stability • Depends mainly on • Rotator cuff muscle, • deltiod & biceps muscles • The weakest part is • the inferior aspect of the capsule( no muscles)
ANTERIOR DISLOCATION • Shoulder joint is the most commonly dislocated large joint • Common type is anterior dislocation (post. Dislocation is very rare) • Young adult(athletes) • Excessive extension and lateral rotation of the humerus • Head of the humerus comes to lie inferior to the glenoidfossa • Head is pulled (by flexors and adductors of the shoulder joint) forward And upward into the subcoracoid position
Elbow Joint TYPE: Hinge type of synovial joint ARTICULATIONS : Trochlea and spheroidalcapitulum of the humerus articulate with the trochlear notch of the ulna and the slightly concave superior aspect of the head of the radius
CAPSULE : The fibrous layer of the joint capsule surrounds the elbow joint. The synovial membrane lines the internal surface of the fibrous layer of the capsule and the intracapsular non-articular parts of the humerus.
Ligaments of the Elbow Joint Lateral: Radial collateral ligament extends from the lateral epicondyle of the humerus and blends distally with the anular ligament of the radius. Medial: Ulnar collateral ligament extends from the medial epicondyle of the humerus to the coronoid process and olecranon of the ulna.
Movements of the Elbow Joint Flexion and extension occur at the elbow joint. Chief flexors of the elbow joint are the brachialis and biceps brachii. Chief extensor of the elbow joint is the triceps brachii.
Bursae around the Elbow Joint 1. Intratendinousolecranon bursa 2. Subtendinousolecranon bursa 3. Subcutaneous olecranon bursa
Bursitis of the Elbow Student's elbow: Subcutaneous olecranon bursa is exposed to injury during falls on the elbow and to infection from abrasions of the skin covering the olecranon.
Tennis elbow(Lateral epicondylitis) • It occurs at the common extensor tendon that originates from the lateral epicondyle. • The acute pain that a person might feel occurs as one fully extends the arm.
Golfer's elbow(medial epicondylitis) • Is an inflammatory condition of the medial epicondyle of the elbow.
Proximal radioulnar joint Type: Pivot type of synovial joint Articulation: Head of the radius articulates with the radial notch of the ulna Ligaments: The strong anular ligament, attached to the ulna anterior and posterior to its radial notch.
Movements Pronation and supination. Pronation: Pronatorquadratus (primarily) and pronatorteres Supination:Supinator and biceps brachii.
Subluxation and Dislocation of Radial Head Pulled elbow or Nursemaid's elbow The sudden pulling of the upper limb tears the distal attachment of the anular ligament, where it is loosely attached to the neck of the radius.
Wrist Joint (radiocarpal) Type: Condyloid (ellipsoid) type of synovial joint Articulation: The ulna does not participate in the wrist joint. The distal end of the radius articulate with the proximal row of carpal bones, except for the pisiform.
Movements of the Wrist Joint Flexion, extension, abduction and adduction (radial deviation and ulnar deviation).
Tendon Reflexes • Deep Tendon Reflexes will not work if either the sensory or motor component of the nerve to the muscle being tested are injured, or if the spinal cord segment where the reflex is integrated is injured.
Biceps jerk Technique : Patient sitting and relaxed. Therapist places her thumb over biceps tendon and applies a brisk tap (to her thumb nail) with reflex hammer Hypo reflex – problem in Nerves or Roots Hyper Reflex – Problem in Spinal cord or Brain
Triceps Jerk It is initiated by the Cervical spinal nerve 7 nerve root ( C7)