Download
1 / 64
650 likes | 801 Views
Antibiotic Approval Program on Patients’ Clinical Outcomes and Antibiotic Expenditures at Siriraj Hospital Pinyo Rattanaumpawan MD Patama Sutha MD Visanu Thamlikitkul MD

E N D
Antibiotic Approval Program on Patients’ Clinical Outcomes and Antibiotic Expenditures at Siriraj Hospital Pinyo Rattanaumpawan MD Patama Sutha MD Visanu Thamlikitkul MD Department of Medicine Faculty of Medicine Siriraj HospitalMahidol University, Bangkok, Thailand
Siriraj Hospital Profile Faculty of Medicine Siriraj Hospital, Mahidol University • Tertiary Care University Hospital in Bangkok • 2,300 Hospital Beds • 2,600,000 Out-patients’ visits per year • 100,000 In-patients per year • 1,400 Physicians (700 residents & clinical fellows)
Background • Thailand National List of Essential Medicines • Drugs in category D should be approved by • qualified specialists and DUE should be • conducted to avoid inappropriate use and • to promote appropriate use of such drugs
Background • Thailand National List of Essential Medicines • Drugs in category D should be approved by • qualified specialists and DUE should be • conductedto avoid inappropriate use and • to promote appropriate use of such drugs • Many antibiotics are listed in category D • including • Piperacillin/Tazobactam • Imipenem • Meropenem • very broad spectrum • last line therapy for • resistant bacteria • very expensive
Background • Cost of Piperacillin/Tazobactam, Imipenem • and Meropenem at Siriraj Hospital in 2006 • ~ $ 4,000,000
Background • Cost of Piperacillin/Tazobactam, Imipenem • and Meropenem at Siriraj Hospital in 2006 • ~ $ 4,000,000 • DUE of these 3 drugs in 2007 revealed that • Inappropriate use at prescription ~ 10% • Inappropriate use at continued treatment (2-3 days after initial prescription) ~50%
Background • Cost of Piperacillin/Tazobactam, Imipenem • and Meropenem at Siriraj Hospital in 2006 • ~ $ 4,000,000 • DUE of these 3 drugs in 2007 revealed that • Inappropriate use at prescription ~ 10% • Inappropriate use at continued treatment (2-3 days after initial prescription) ~50% • Hospital administrators were concerned on • inappropriate use and cost of these 3 drugs
Background • Siriraj Hospital decided to have antibiotic • approval measure and DUE of these 3 drugs • according to recommendation of Thailand • National List of Essential Medicines
Background • Siriraj Hospital decided to have antibiotic • approval measure and DUE of these 3 drugs • according to recommendation of Thailand • National List of Essential Medicines • Responsible physicians raised a concern on • negative effect of this measure on clinical • outcomes for patients whose antibiotics are • changed or discontinued
Background • Siriraj Hospital decided to have antibiotic • approval measure and DUE of these 3 drugs • according to recommendation of Thailand • National List of Essential Medicines • Responsible physicians raised a concern on • negative effect of this measure on clinical • outcomes for patients whose antibiotics are • changed or discontinued • No solid evidence from literature to support such negative effect
Background • Siriraj Hospital decided to have antibiotic • approval measure and DUE of these 3 drugs • according to recommendation of Thailand • National List of Essential Medicines • Responsible physicians raised a concern on • negative effect of this measure on clinical • outcomes for patients whose antibiotics are • changed or discontinued • No solid evidence from literature to support such negative effect • Siriraj Hospital endorsed a study to convince • responsible physicians on patients’ outcomes
Objective • To determine effectiveness of antibiotic • approval measure on patients’ clinical • outcomes and antibiotic expenditures
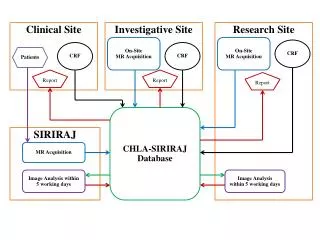
Methods • Randomized controlled study in hospitalized • adult patients who received piperacillin/ • tazobactam, imipenem and meropenem from • August to November 2007
Methods • Randomized controlled study in hospitalized • adult patients who received piperacillin/ • tazobactam, imipenem and meropenem from • August to November 2007 • Once there was a prescription of any target antibiotics, Pharmacy Department notified study team • Study team allocated the target antibiotic • prescription to either control group or • antibiotic approval group by simple • randomization
Methods • Control Group • Patients received antibiotics according to • their physicians’ decision • Study team observed patients’ clinical • courses and outcomes until the patients left • the hospital
Methods • Antibiotic Approval Group • Patients were assessed by infectious disease • specialist to determine if target antibiotics • were indicated according to predetermined • criteria
Predetermined Criteria • Piperacillin/Tazo., Imipenem, Meropenem • Confirmed or suspected P.aeruginosa infection • Infection due to pathogen resistant to • cephalosporins, aminoglycosides, quinolones • Empiric therapy for neutropenic fever • Infection due to pathogen susceptible to other antibiotics but the patient is unable to receive such antibiotics
Predetermined Criteria • Additional criteria forimipenem & meropenem • Therapy of nosocomial infection which is not responding to other antibiotics • Infection due to pathogen which is resistant to beta-lactam + beta-lactamase inhibitor • Severe infection due to ESBL+ve pathogen
Methods • Antibiotic Approval Group • Patients were assessed by infectious disease • specialist to determine if target antibiotics • were indicated according to predetermined • criteria • If target antibiotic was indicated, it was continued • If target antibiotic was not indicated, study • team suggested stopping or modifying it
Methods • Antibiotic Approval Group • Patients were assessed by infectious disease • specialist to determine if target antibiotics • were indicated according to predetermined • criteria • If target antibiotic was indicated, it was continued • If target antibiotic was not indicated, study • team suggested stopping or modifying it • Study team observed patients’ clinical • courses and outcomes until the patients left • the hospital
Clinical Outcomes • Favorable outcomes : Cure & Improvement • Eradication of causative pathogens • Length of hospital stay • Duration of fever • Side effects of antibiotics • Death due to infection • Status at discharge
Antibiotic Consumption & Expenditure • Duration of all antibiotics • Duration of target antibiotics • Total cost of all antibiotics • Total cost of target antibiotics • Defined Daily Dose (DDD) of all antibiotics • DDD of target antibiotics
Methods • Sample Size • Non-inferiority study • Favorable outcome in control gr. = 70% • Favorable outcome in intervention group was < 5% of control group • Type I error 5% and Type II error 20% • 500 prescriptions in each group
Results • 1,028 prescriptions of imipenem, meropenem, • piperacillin/tazobactam in 948 patients • 516 prescriptions (486 patients) - Control • 512 prescriptions (462 patients) - Intervention
Characteristics of Patients • Characteristic Control Intervention p (N=516) (N=512) • Males 52.9% 53.0% 0.9 • Mean Age 62.1 y. 63.5 y. 0.2 • Location of Patients • Medical Wards 68.9% 70.8% 0.7 • Surgery Wards 25.1% 24.5% • Type of Infections • CAI 18.0% 20.9% 0.2 • HAI 82.0% 79.1%
Characteristics of Patients • Characteristic Control Intervention p (N=516) (N=512) • Purpose of Antibiotic Usage • Treatment 98.6% 98.6% 1 • Prophylaxis 1.4% 1.4% • Type of Target Antibiotic • Pip./Tazobac. 46.9% 44.5% 0.6 • Imipenem 35.4% 35.7% • Meropenem 17.6% 19.7%
Inappropriate Prescriptions • 42% of target antibiotic prescriptions were • considered inappropriate
Compliance to Suggestions • 42% of target antibiotic prescriptions were • considered inappropriate • 46% of inappropriate prescriptions were changed to more appropriate antibiotics according to suggestions
Compliance to Suggestions • 42% of target antibiotic prescriptions were • considered inappropriate • 46% of inappropriate prescriptions were changed to more appropriate antibiotics according to suggestions • 24% of inappropriate prescriptions were discontinued according to suggestions (antibiotics were not needed)
Compliance to Suggestions • 42% of target antibiotic prescriptions were • considered inappropriate • 46% of inappropriate prescriptions were changed to more appropriate antibiotics according to suggestions • 24% of inappropriate prescriptions were discontinued according to suggestions • 22% of inappropriate prescriptions were changed to other inappropriate antibiotics not suggested by infectious disease specialist (non-compliance rate & squeezing the balloon)
Outcomes of Patients Clinical Outcome Control Intervention p (N=516) (N=512)Favorable Outcome 60.5% 68.9% <0.01 Eradicate Pathogens 50.2% 65.4% <0.01 Mean LOS 30.7 d. 30.4 d. 0.8 Mean Length Fever 11.0 d. 7.5 d. <0.01 Antibiotic Allergy 1.4% 0.4% 0.1 AAD 3.5% 4.9% 0.2Death from Infection 35.4% 29.4% 0.05 Mean d. all ATB 16.4 d. 12.7 d. <0.01 Mean d. target ATB 9.3 d. 7.5 d. <0.01Alive at Discharge 57.4% 55.6% 0.6
Outcomes of Patients Clinical Outcome Control Intervention p (N=516) (N=512)Favorable Outcome 60.5% 68.9% <0.01 Eradicate Pathogens 50.2% 65.4% <0.01 Mean LOS 30.7 d. 30.4 d. 0.8Mean Length Fever 11.0 d. 7.5 d. <0.01 Antibiotic Allergy 1.4% 0.4% 0.1 AAD 3.5% 4.9% 0.2 Death from Infection 35.4% 29.4% 0.05 Mean d. all ATB 16.4 d. 12.7 d. <0.01 Mean d. target ATB 9.3 d. 7.5 d. <0.01 Alive at Discharge 57.4% 55.6% 0.6
Antibiotic Consumption & Expenditure Control Intervention (N=516) (N=512) Total Cost all ATB (m.$) 0.71 0.54 Total Cost target ATB (m.$) 0.34 0.28 All ATB/Episode ($) 1,238 967 Target ATB/Episode ($) 661 538 DDD all ATB 13,528 10,738 DDD target ATB 3,696 2,972 DDD all ATB/Episode 26.2 21.0 DDD target ATB/Episode 7.2 5.8
Antibiotic Consumption & Expenditure Control Intervention (N=516) (N=512) Total Cost all ATB (m.$) 0.71 0.54 Total Cost target ATB (m.$) 0.34 0.28 All ATB/Episode ($) 1,238 967 Target ATB/Episode ($) 661 538 DDD all ATB 13,528 10,738 DDD target ATB 3,696 2,972 DDD all ATB/Episode 26.2 21.0 DDD target ATB/Episode 7.2 5.8 Minimal “Squeezing the Balloon Effect”
Antibiotic Consumption & Expenditure • Actual difference in antibiotic expenditures between antibiotic approval group and control group was $ 143,793 • Annual antibiotic cost savings from antibiotic approval program would be $ 862,704 if all prescriptions of target antibiotics were reviewed by infectious disease physicians
Conclusion Antibiotic approval program for imipenem, meropenem, piperacillin/tazobactam at Siriraj Hospital is an effective measure in reducing antibiotic consumption & expenditurewithout compromising patients’ clinical outcomes
Cost-Benefit of Antibiotic Approval Program • If all prescriptions of target antibiotics are reviewed by infectious diseases physicians, hospital will have annual saving US $ 862,704 • Extra costs of DUE and antibiotic approval processes are not taken into account when aforementioned amount of cost savings is estimated • Extra costs generated by DUE and antibiotic approval (personnel costs and additional costs for microbiologic investigations) are estimated as up to US $ 50,000 per year • DUE & antibiotic approval are cost-benefit
Prerequisite of Antibiotic Approval Program • Antibiotic approval can be applied only to institutions where there are qualified infectious diseases physicians who are willing to take responsibility in approving restricted antibiotics and are able to continue providing suggestions regarding antibiotic prescription and management of infections
Prerequisite of Antibiotic Approval Program • Antibiotic approval can be applied only to institutions where there are qualified infectious diseases physicians who are willing to take responsibility in approving restricted antibiotics and are able to continue providing suggestions regarding antibiotic prescription and management of infections • Well trained clinical pharmacists should be able to perform approval
Implementations • Study results were presented to hospital administrators in April 2008 • Siriraj Hospital informed all responsible physicians regarding the study results • Antibiotic approval measure has been continued since May 2008
More Information • Poster Number 291 • American Journal of Infection Control • 2010; 38: 38 - 43.
Antibiotic Approval Program on Patients’ Clinical Outcomes and Antibiotic Expenditures at Siriraj Hospital Pinyo Rattanaumpawan MD Patama Sutha MD Visanu Thamlikitkul MD Department of Medicine Faculty of Medicine Siriraj HospitalMahidol University, Bangkok, Thailand
Characteristics of Patients Characteristic Control Intervention p (N=516) (N=512) Underlying Conditions of Patients Cardio-pulmonary 38.7% 54.1% <0.01Malignancy 34.0% 42.0% 0.01 Liver Diseases 6.6% 11.7% 0.01 Renal Diseases 16.3% 22.3% 0.02 Neurological Dis. 15.4% 22.9%0.01
Clinical Outcomes of Patients • Different characteristics between 2 groups • Multivariate analysis was performed • Factors associated with unfavorable outcome • OR (95%CI) p • Control group patient 1.35 (1.03-1.76) 0.03 • Pneumonia 2.36 (1.78-3.15) <0.01
Impact of Antibiotic Approval Program on Antimicrobial Resistance • Impact on antibiotic resistance of pathogens was not measured because patients allocated to both groups stayed in the same wards, and duration of study was only 4 months • Therefore, it would be unlikely to observe any changes in antibiotic resistance patterns • of isolated pathogens either from patients or • from environment • There are many factors contributing to AMR
Subgroup Analysis in Microbiological Documented Infections Clinical Outcome Control Intervention p (N=290) (N=323) Favorable Outcome 58.9% 65.6% 0.08 Eradicate Pathogen 50.2% 65.4% <0.01 Death (Infection) 37.9% 31.9% 0.1
Main Reasons for Non-Compliance • Responsible physicians did not believe that patient was free of active infection according to infectious disease physician’s opinion • Some surgeons believed that antibiotic prophylaxis should be continued until endotracheal tube was removed • Many responsible physicians were not certain that narrow spectrum antibiotics could replace target antibiotics that they initially gave to their patients, especially for the patients who were improving after receiving the target antibiotics
Different Rates of Comorbidity • Infectious diseases physicians did not involve in care processes in control group whereas • infectious diseases physicians continued supervising management of patients who received antibiotic approval • Additional medical information was recorded, and additional microbiologic • investigations for diagnosis of infections and for assessment of microbiologic outcomes were made for antibiotic approval group
Different Rates ofComorbidity • Differences in characteristics of patients would not favor outcomes of patients who received antibiotic approval because higher rates of having comorbidity that compromised clinical outcomes were observed more often in patients who received antibiotic approval
Inappropriate Use of Target Antibiotics • Prevalence of inappropriate use of target antibiotics in antibiotic approval group was 41.6% which was modestly less than 50% observed from a preliminary DUE period • This might be due to each prescription of target antibiotics during study period was required to be accompanied with antibiotic order sheet that was filled in by responsible physician • Therefore, some prescriptions of target antibiotics were cancelled earlier if responsible physicians thought that their prescriptions were obviously inappropriate