Download
1 / 1
10 likes | 198 Views
THE FULLY ENDOSCOPIC SUPRAORBITAL APPROACH. Mohamed S. Kabil, MD Hrayr K. Shahinian, MD, FACS. Introduction

E N D
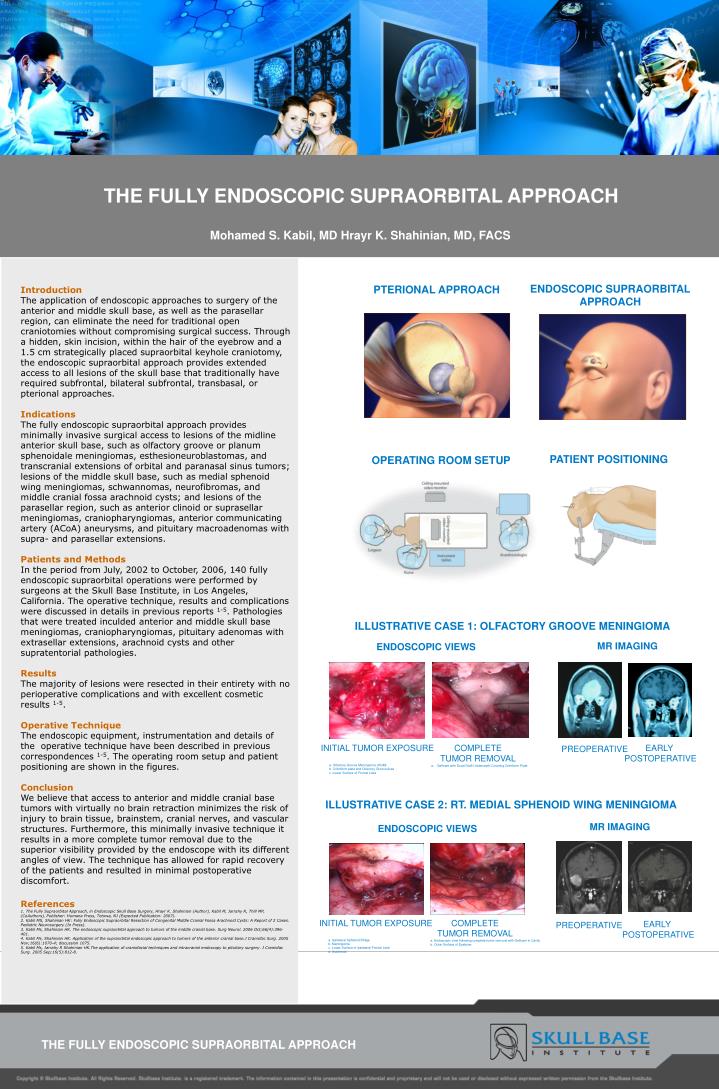
THE FULLY ENDOSCOPIC SUPRAORBITAL APPROACH Mohamed S. Kabil, MD Hrayr K. Shahinian, MD, FACS Introduction The application of endoscopic approaches to surgery of the anterior and middle skull base, as well as the parasellar region, can eliminate the need for traditional open craniotomies without compromising surgical success. Through a hidden, skin incision, within the hair of the eyebrow and a 1.5 cm strategically placed supraorbital keyhole craniotomy, the endoscopic supraorbital approach provides extended access to all lesions of the skull base that traditionally have required subfrontal, bilateral subfrontal, transbasal, or pterional approaches. Indications The fully endoscopic supraorbital approach provides minimally invasive surgical access to lesions of the midline anterior skull base, such as olfactory groove or planum sphenoidale meningiomas, esthesioneuroblastomas, and transcranial extensions of orbital and paranasal sinus tumors; lesions of the middle skull base, such as medial sphenoid wing meningiomas, schwannomas, neurofibromas, and middle cranial fossa arachnoid cysts; and lesions of the parasellar region, such as anterior clinoid or suprasellar meningiomas, craniopharyngiomas, anterior communicating artery (ACoA) aneurysms, and pituitary macroadenomas with supra- and parasellar extensions. Patients and MethodsIn the period from July, 2002 to October, 2006, 140 fully endoscopic supraorbital operations were performed by surgeons at the Skull Base Institute, in Los Angeles, California. The operative technique, results and complications were discussed in details in previous reports 1-5. Pathologies that were treated inculded anterior and middle skull base meningiomas, craniopharyngiomas, pituitary adenomas with extrasellar extensions, arachnoid cysts and other supratentorial pathologies. Results The majority of lesions were resected in their entirety with no perioperative complications and with excellent cosmetic results 1-5. Operative Technique The endoscopic equipment, instrumentation and details of the operative technique have been described in previous correspondences 1-5. The operating room setup and patient positioning are shown in the figures. ConclusionWe believe that access to anterior and middle cranial base tumors with virtually no brain retraction minimizes the risk of injury to brain tissue, brainstem, cranial nerves, and vascular structures. Furthermore, this minimally invasive technique it results in a more complete tumor removal due to the superior visibility provided by the endoscope with its different angles of view. The technique has allowed for rapid recovery of the patients and resulted in minimal postoperative discomfort. References 1. The Fully Supraorbital Approach, in Endoscopic Skull Base Surgery, Hrayr K. Shahinian (Author), Kabil M, Jarrahy R, Thill MP, (CoAuthors), Publisher: Humana Press, Totowa, NJ (Expected Publication: 2007). 2. Kabil MS, Shahinian HK: Fully Endoscopic Supraorbital Resection of Congenital Middle Cranial Fossa Arachnoid Cysts: A Report of 2 Cases. Pediatric Neurosurgery (In Press). 3. Kabil Ms, Shahinian HK. The endoscopic supraorbital approach to tumors of the middle cranial base. Surg Neurol. 2006 Oct;66(4):396-401. 4. Kabil Ms, Shahinian HK. Application of the supraorbital endoscopic approach to tumors of the anterior cranial base.J Craniofac Surg. 2005 Nov;16(6):1070-4; discussion 1075. 5. Kabil Ms, Jarrahy R Shahinian HK.The application of craniofacial techniques and intracranial endoscopy to pituitary surgery. J Craniofac Surg. 2005 Sep;16(5):812-8. ENDOSCOPIC SUPRAORBITAL APPROACH PTERIONAL APPROACH PATIENT POSITIONING OPERATING ROOM SETUP ILLUSTRATIVE CASE 1: OLFACTORY GROOVE MENINGIOMA MR IMAGING ENDOSCOPIC VIEWS INITIAL TUMOR EXPOSURE COMPLETE TUMOR REMOVAL EARLY POSTOPERATIVE PREOPERATIVE a.Gelfoam with Dural Graft Underneath Covering Cribriform Plate a. Olfactory Groove Meningioma (OGM) b. Cribriform plate and Olfactory Groove Area c. Lower Surface of Frontal Lobe ILLUSTRATIVE CASE 2: RT. MEDIAL SPHENOID WING MENINGIOMA MR IMAGING ENDOSCOPIC VIEWS INITIAL TUMOR EXPOSURE COMPLETE TUMOR REMOVAL EARLY POSTOPERATIVE PREOPERATIVE a. Ipsilateral Sphenoid Ridge b. Meningioma c. Lower Surface of ipsilateral Frontal Lobe d. Arachnoid a. Endoscopic view following complete tumor removal with Gelfoam in Cavity b. Outer Surface of Eyebrow THE FULLY ENDOSCOPIC SUPRAORBITAL APPROACH