Download
1 / 45
450 likes | 607 Views
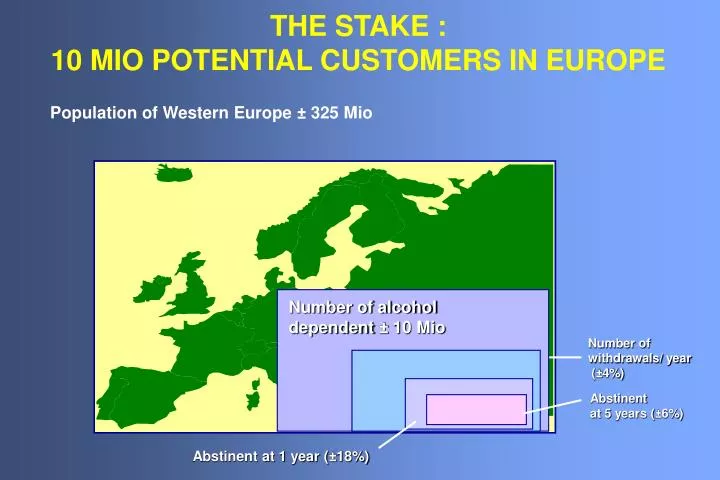
THE STAKE : 10 MIO POTENTIAL CUSTOMERS IN EUROPE. Population of Western Europe ± 325 Mio. Number of alcohol dependent ± 10 Mio. Number of withdrawals/ year (±4%). Abstinent at 5 years (±6%). Abstinent at 1 year (±18%).

E N D
THE STAKE : 10 MIO POTENTIAL CUSTOMERS IN EUROPE Population of Western Europe ± 325 Mio Number of alcohol dependent ± 10 Mio Number of withdrawals/ year (±4%) Abstinent at 5 years (±6%) Abstinent at 1 year (±18%)
STATES OF CHANGE - REVOLVING DOOR MODEL(Di Clemente et Prochaska, 1982) Précontemplation Relapse Contemplation Maintenance Préparation Action Décision
TYPES OF CRAVING: DEFINITIONS • Psychological craving: • Strong desire for drinking alcohol • Strong, almost overpowering urge for alcohol during acute withdrawal • Strong desire or sense of compulsion to take alcohol (ICD-10) • Persistent desire or unsuccessful efforts to cut down or control alcohol use (DSM-IV) • Physical craving: • Elevated heart rate, • Sweeting, • Nausea, • Anxiety
MANY STIMULI PRECEDE THE ARRIVAL OF ALCOHOL INSIDE THE BRAIN Sights and sounds of the environment Smell of alcohol etc. Taste of alcohol BAR
HOW CONDITIONED STIMULI BECOMESCUES FOR RELAPSE? This is our patient, he/she has been detoxified and has turned his/her back on alcohol and all the associated stimuli. Unfortunately, in our alcohol-based society it is impossible to avoid all these stimuli for long. BAR Each cue initiates adaptation inside the brain BAR
HOW CONDITIONED STIMULI BECOME CUES FOR RELAPSE Any of these stimuli induce adaptation which produces feelings opposite to those of alcohol eg anxiety, dysphoria. These feelings can be self-medicated with alcohol but the decision to do so intensifies all the cues. BAR BAR BAR alcohol In order to balance the increasingly severe "pseudo-withdrawal produced by the conditioned adaptation the patient relapses into heavy drinking
PAVLOVIAN CONDITIONING AND THE EFFECTS OF ALCOHOL BAR ALCOHOL Unconditioned stimulus BAR Associated stimuli As the associated stimuli repeatedly precede the arrival of alcohol in the brain "conditioning" occurs BAR Conditioned stimuli Response Once the stimuli have become conditioned they elicit the response (eg feelings of relaxation) even before the alcohol arrives in the brain BAR
BAR EACH TIME THE ALCOHOL ARRIVES THE BRAIN INITIATES INCREASINGLY EFFECTIVE CHEMICAL ADAPTATIONS WHICH OPPOSE THE DRUG AND CAUSE TOLERANCE BAR BAR BAR But every time the adaptation is preceded by the associated stimuli and so these become conditioned stimuli capable of eliciting the adaptation even before the alcohol arrives BAR BAR ONE CONSEQUENCE IS THAT TOLERANCE IS USUALLY GREATER IN A FAMILIAR ENVIRONMENT BECAUSE THE "CUES" HELP INITIATE THE ADAPTATION TO ALCOHOL INSIDE THE BRAIN
RELATIONSHIP BETWEEN THE SEVERITY OF ALCOHOL PROBLEMS AND THE TYPE OF INTERVENTION NEEDED None Mild Moderate Substantial Severe ALCOHOL PROBLEMS Specialized treatment Brief intervention Primary prevention From: Heather (1995) Source: Institute of Medicine (1990)
EFFECTIVE PSYCHOLOGICAL TREATMENT FOR DRINKING PROBLEMS • Motivational interviewing • Cognitive - behaviour theory • Relapse prevention • Community reinforcement
Campral® AND GLUTAMATE % Baseline level 0 1 2 3 4 5 6 7 8 9 10 11 12 13 Time (hr) after withdrawal p < 0.001 Ref: De Witte Progress in Neurobiology. 2000, 343-362
WITHDRAWAL P < 0.05 Motility / Rat / 12h Ref: De Witte
ACAMPROSATE • No effect on non-alcohol-preferring and non-dependent animals • Abolishes the alcohol dependence in dependent animals • Abolishes the alcohol withdrawal • Keeps dependent animals alive during multiple successive withdrawals Ref: De Witte presentation
MATERIAL Combined Data Analysis • 11 Double blind, placebo controlled multicentre studies • 8 European countries • 3 338 alcohol dependent patients Mean Age 42.8 years ± 9.3 Sex: female 19% Mean MAST score 31.8 ± 10.9 Mean CAGE score 3.5 ± 0.76
METHODOLOGY 1 • Data of all 11 trials were reasonably comparable for criteria which included: • demographic variables • clinical histories • the major efficacy outcome criteria • Safety data were readily comparable for 9 studies • Treatment Duration: 3 months in one trial, 6 months in 5 trials and 12 months in 5 trials • Medication free follow-up periods varied from 4 weeks to 12 months • Assessment intervals during treatment differed Common data were identified at days 0, 30, 90, 180, 270, 360
METHODOLOGY 2 Comparability • All placebo controlled trials, performed under naturalistic conditions • Two treatment groups (acamprosate and placebo) in 9 trials; three treatment groups (two acamprosate groups at different dosages and one placebo group) in 2 trials. 4-6 tablets per day • All patients were started on study medication after the period of acute detoxification: • 10 trials immediately after acute withdrawal therapy, all patients abstinent at start of treatment • 1 trial within 6 weeks of termination of acute withdrawal therapy, 60% patients abstinent
METHODOLOGY 3 • To follow a CORE PROTOCOL ± adaptations according countries’ requests • Studies carried out in accordance with the EUROPEAN GOOD CLINICAL PRACTICE • To use CENTRAL LABORATORY FACILITIES (PRAMA, UKMAS) or to standardise the laboratory values • PRIMARY OUTCOME CRITERION: Drinking behaviour 1- Abstinence/Relapse/Missing assessment at each visit 2- Time to first relapse (survival analysis) 3- Cumulative Abstinence Duration (a mathematical sum of all abstinent periods)
OUTCOME CRITERIA Number of dry days: cumulative abstinence duration (CAD) If exact data were available: cumulate directly Time to First Relapse = 30 days Cumulative Abstinence Duration = 75 days Relapses CAD D0 D30 D60 D90 D120 D150 D180 If exact data were not available: consider total period between visits Cumulative Abstinence Duration = 60 days Relapses CAD Visit 1 2 3 4 5 6 7
OUTCOME CRITERIA • At each visit: drinking or not? • Time to first drink Alcohol consumption (quantity) D0 D30 D60 D90 D120 D150 D180 Assessment visits A A R R A A R A = abstinence R = relapse
EUROPEAN TRIALS: RATE OF TOTAL ABSTINENCE (%) 2 way ANOVA - treatment: p<0.001, study: p<0.001, interact: NS
RESULTS: ABSTINENT RATE Survival analysis % Mantel Cox: p<0.001 %Abstinence rate (no alcohol consumption) Days • It measures: • time to first relapse • absolute abstinence • Comment: this method does not take subsequent abstinent periods • into consideration, but is a conservative measure to assess outcome
RESULTS: PROPORTION OF ATTENDING PATIENTS * * * * Attendance rate (%) Days Differential attrition between treatment groups Comment: drop-out rate in naturalistic trials could be an objective outcome measure of efficacy
RESULTS: ABSTINENCE RATE PER VISIT *: p<0,001 * * Abstinence rate (%) * * * Days
SF 36 QoL SCORES BEFORE AND AFTER CAMPRAL TREATMENT Before Treatment After Campral® Treatment Physical Component Mental Component PFPhysical Functioning BPBodily pain RPRole Physical GHGeneral Health MHMental Health SFSocial Funtioning RERole Emotional VTVitality HTHealth Transition
CONCLUSIONS FROM Campral®CLINICAL STUDIES • Double the abstinence rates compared with placebo • Used within a programme of psychosocial support, Campral® can significantly improve abstinence rates following alcohol withdrawal • Campral® is equally effective with a range of psychosocial support strategies
RESULTS: ADVERSE EVENTS Adverse events of statistical significance with a frequency of more than 5% were: Gastro-intestinal irritation 15% in the first 30 days, 8% d31-90 4-8% more than placebo Sex drive changes 9% in the first 30 days 3% more than placebo Difficulty in falling asleep 7% between days 181 and 270 3% more than placebo GOOD SAFETY PROFILE
Campral®: A MAJOR ADVANCE IN THE TREATMENT OF CHRONIC ALCOHOLISM • A novel and unique non-aversive therapeutic agent • Abstinence rates twice that with placebo achieved when used in conjunction with psycho-social support measures • Good tolerability established • No significant dependence potential
MICADO STUDY (Netherlands) De Wildt et al (submitted for publication) • 248 Patients • 28 weeks Campral treatment for all patients (4-6 tablets / day) • 3 Treatment Groups with different levels of counselling • Manual driven • Session recordings
MICADO STUDY (Netherlands) De Wildt et al • 3Treatment Groups • a) Campral only: • 6 weekly~ 10 min medical visits. Collect drinking data, evaluate vital signs • no reinforcement, motivation, high risk situation discussions. • b) Campral with Minimal Intervention (MI) a plus: • 3 x 20 min weekly visits (W 2, 3, 4) • discuss cost benefit drinking • discuss drinking situations • review motivation • c) Campral with Brief Psycho-Social Intervention (PSI) a plus: • 7 x 60 min weekly visits (W 2, 3, 4, 5, 6, 7, 8) • Increase coping skills (Monti, Abrams et al 89, MATCH-Kadden 92, Schippers 94) • significant other, good and bad moments, problem solving, cognitive restructuring
MICADO STUDY (Netherlands) De Wildt et al
CONCLUSIONS • 14 out of 17 studies confirmed that acamprosate reduces relapse in alcohol dependence. • Treatment over 12 months suggests continued abstinence after termination of medication. • Adverse events are rare and minor. • Early evidence suggests that acamprosate without particular psycho-social support may be as effective as acamprosate combined with minimal or brief intervention. Further investigation is necessary.
ACAMPROSATE AND QUALITY OF LIFE HRQoL secondary analysis of the European NEAT Programme Synthesis from 5 countries: Austria, Belgium, Portugal, Switzerland and the United Kingdom F. Poldrugo, Department of Psychiatry, University of Trieste, Italy P. Lehert, Catholic University of Mons, Belgium Main Investigators: C. Ansoms, F. Fisher, W.J. Fuchs, M. Morgan, I. Pelc and A.J. Pires Preto
CAPRISO STUDY Study design • Primary objectives: • Comparison of the efficacy of acamprosate with or without a • follow-up by a social nurse after detoxification • Study design: • The patients were hospitalized for 3 weeks and randomized to one of the 2 treatment groups • Group 1: The patient sees his/her GP whenever necessary. However, the follow-up is monitored by a nurse • Group 2: The patient is seen by his/her GP • Treatment duration: • 26 weeks
CAPRISO STUDY • Methods (1) • Prospective evaluation during a 26 weeks follow-up period of alcoholic patients, after detoxification • Two randomized parallel groups with follow-up by a social nurse (F group, N = 50) or without follow-up (NF group, N = 50) • Evaluation visit at week 1, 2, 3, 4, 6, 10, 14, 18, 22, 26 • Outpatient from week 4 • Acamprosate for all patients
CAPRISO STUDY • Methods (2) • Evaluation of efficacy: • For every visit, the patient is considered as abstainer, relapser or missing. • Missing = relapser • Outcome criteria: • Main endpoint: CAD (sum of complete abstinent days) * Second endpoints: CGI and compliance • Statistical analysis: Anova on ranks • Explanatory analysis: GLM on ranks • A priori Power: n = 2*50 / =.05 =.2 = 25% 2 - sided
CAPRISO STUDY Population (N = 100) - Exclusion Criteria • Other dependencies except nicotine • An expected longer hospital stay more than 3 weeks for detoxification • Known renal insufficiency • Previous treatment with acamprosate • Having participated in another study in the last 30 days • Pregnancy or breast feeding in women of childbearing age • Legal incapacity
CAPRISO STUDY Population (N = 100) - Inclusion Criteria • Men and women from 18 to 65 years old • DSM-IV criteria for alcohol dependence • Last alcohol consumption within the previous 7 days • Undergoing an inpatient detoxification planned for 3 weeks • Living in the region of Brussels • Having given written informed consent
CAPRISO STUDY Baseline data per type of follow up
CAPRISO STUDY Population (N = 100) - Demographic Data Age (years) 43.3 8.2 Gender female (%) 22 Marital status (%) Education status (%) Family history (%) 63 Smoking (%) 82 Employement (%)
CAPRISO STUDY Influence of baseline variables on CAD % Cont’d No evident effect observed with Initial Severity Living status Smoking habits Drinking pattern Number of previous withdrawal
CAPRISO STUDY Clinical Global Impression 2: p = 0.011
CAPRISO STUDY Conclusion 1. Significant differences in outcomes between the 2 treatment conditions showing a strong influence of social nurse intervention during psycho-social follow-up 2. Success rate of the pharmacological active treatment (Acamprosate, I. Pelc, 1992) is positively or negatively influenced by a psycho-social support process 3. Significant influence of Age, Education, Marital status, Family History, Gender and Previous Attendance to SHG on CAD 4. No significant influence of Smoking, Drinking Pattern, Living Status, Number of Previous Detoxification and Initial Severity 5. Providing psycho-social support has to be relevant to patient’s specific needs
CAPRISO STUDY I. PELC, M.D., Ph.D. Collaborators P. Verbanck M.D, Ph. D. O. Le BON M.D. Psychiatrists C. Hanak M.D. J. Tecco M.D. A. Vandenborre Chief Nurse D. Montag, S. Minet Social Workers M. Streel, X. Noël B.Sc. Psychologists C. Houtain, I. Baert Social Nurse Researchers Université Libre de Bruxelles Clinical Department and Laboratory of Psychological Medecine, Alcohology and Drug Dependence and General Practitioners of the Brussels’ Region Dr F. Deckers Merck - Lipha - Bruxelles Dr F. Landron Merck - Lipha - Lyon Prof. P. Lehert University of Mons (Belgium) and University of Melbourne (Australia) - Statistical Analysis