Download
1 / 1
10 likes | 89 Views
Psychoeducational Intervention for Women’s Low Sexual Desire and Arousal: Applications of Mindfulness Katherine Rhodes, MA, Lori Brotto, PhD, & Yvonne Erskine, MEd Department of Gynaecology, University of British Columbia, Vancouver, Canada. INTRODUCTION.

E N D
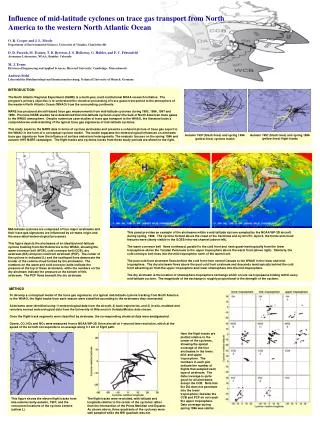
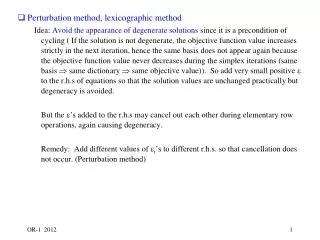
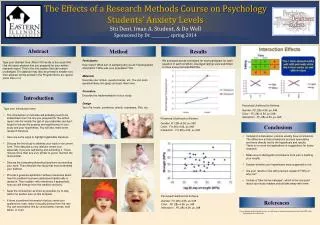
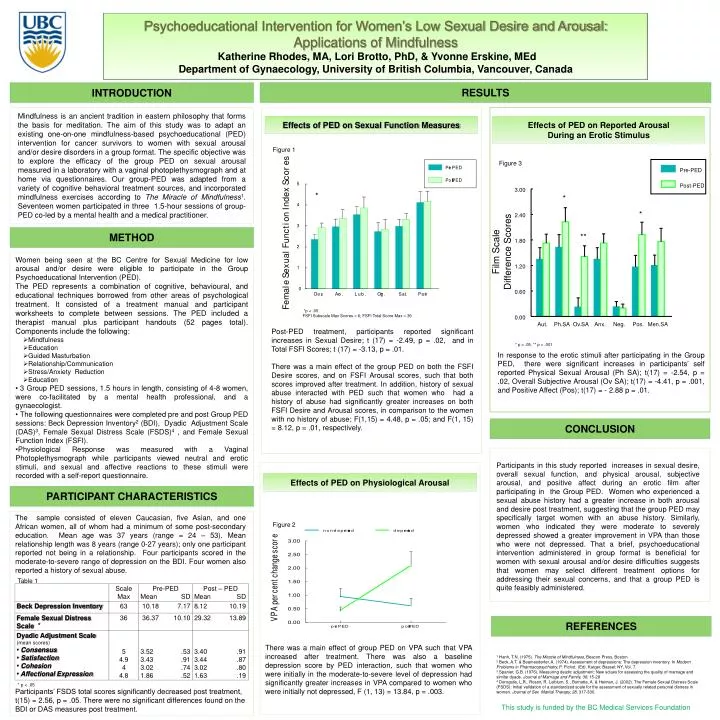
Psychoeducational Intervention for Women’s Low Sexual Desire and Arousal: Applications of Mindfulness Katherine Rhodes, MA, Lori Brotto, PhD, & Yvonne Erskine, MEd Department of Gynaecology, University of British Columbia, Vancouver, Canada INTRODUCTION Mindfulness is an ancient tradition in eastern philosophy that forms the basis for meditation. The aim of this study was to adapt an existing one-on-one mindfulness-based psychoeducational (PED) intervention for cancer survivors to women with sexual arousal and/or desire disorders in a group format. The specific objective was to explore the efficacy of the group PED on sexual arousal measured in a laboratory with a vaginal photoplethysmograph and at home via questionnaires. Our group-PED was adapted from a variety of cognitive behavioral treatment sources, and incorporated mindfulness exercises according to The Miracle of Mindfulness1. Seventeen women participated in three 1.5-hour sessions of group-PED co-led by a mental health and a medical practitioner. Pre-PED Post-PED 3.00 2.40 1.80 Film Scale Difference Scores 1.20 0.60 0.00 Aut. Ph.SA Ov.SA Anx. Neg. Pos. Men.SA RESULTS Effects of PED on Sexual Function Measures Effects of PED on Reported Arousal During an Erotic Stimulus Figure 1 Figure 3 * * * * * ** METHOD ** • Women being seen at the BC Centre for Sexual Medicine for low arousal and/or desire were eligible to participate in the Group Psychoeducational Intervention (PED). • The PED represents a combination of cognitive, behavioural, and educational techniques borrowed from other areas of psychological treatment. It consisted of a treatment manual and participant worksheets to complete between sessions. The PED included a therapist manual plus participant handouts (52 pages total). Components include the following: • Mindfulness • Education • Guided Masturbation • Relationship/Communication • Stress/Anxiety Reduction • Education • 3 Group PED sessions, 1.5 hours in length, consisting of 4-8 women, were co-facilitated by a mental health professional, and a gynaecologist. • The following questionnaires were completed pre and post Group PED sessions: Beck Depression Inventory2 (BDI), Dyadic Adjustment Scale (DAS)3, Female Sexual Distress Scale (FSDS)4 , and Female Sexual Function Index (FSFI). • Physiological Response was measured with a Vaginal Photoplethysmograph while participants viewed neutral and erotic stimuli, and sexual and affective reactions to these stimuli were recorded with a self-report questionnaire. • *p < .05 • FSFI Subscale Max Scores = 6; FSFI Total Score Max = 36 Post-PED treatment, participants reported significant increases in Sexual Desire; t (17) = -2.49, p = .02, and in Total FSFI Scores; t (17) = -3.13, p = .01. There was a main effect of the group PED on both the FSFI Desire scores, and on FSFI Arousal scores, such that both scores improved after treatment. In addition, history of sexual abuse interacted with PED such that women who had a history of abuse had significantly greater increases on both FSFI Desire and Arousal scores, in comparison to the women with no history of abuse; F(1,15) = 4.48, p = .05; and F(1, 15) = 8.12, p = .01, respectively. * p < .05, ** p < .001 In response to the erotic stimuli after participating in the Group PED, there were significant increases in participants’ self reported Physical Sexual Arousal (Ph SA); t(17) = -2.54, p = .02, Overall Subjective Arousal (Ov SA); t(17) = -4.41, p = .001, and Positive Affect (Pos); t(17) = - 2.88 p = .01. CONCLUSION Participants in this study reported increases in sexual desire, overall sexual function, and physical arousal, subjective arousal, and positive affect during an erotic film after participating in the Group PED. Women who experienced a sexual abuse history had a greater increase in both arousal and desire post treatment, suggesting that the group PED may specifically target women with an abuse history. Similarly, women who indicated they were moderate to severely depressed showed a greater improvement in VPA than those who were not depressed. That a brief, psychoeducational intervention administered in group format is beneficial for women with sexual arousal and/or desire difficulties suggests that women may select different treatment options for addressing their sexual concerns, and that a group PED is quite feasibly administered. Effects of PED on Physiological Arousal PARTICIPANT CHARACTERISTICS The sample consisted of eleven Caucasian, five Asian, and one African women, all of whom had a minimum of some post-secondary education. Mean age was 37 years (range = 24 – 53). Mean relationship length was 8 years (range 0-27 years); only one participant reported not being in a relationship. Four participants scored in the moderate-to-severe range of depression on the BDI. Four women also reported a history of sexual abuse. Figure 2 Table 1 REFERENCES * There was a main effect of group PED on VPA such that VPA increased after treatment. There was also a baseline depression score by PED interaction, such that women who were initially in the moderate-to-severe level of depression had significantly greater increases in VPA compared to women who were initially not depressed, F (1, 13) = 13.84, p = .003. 1 Hanh, T.N. (1975). The Miracle of Mindfulness, Beacon Press, Boston. 2 Beck, A.T. & Beamesderfer, A. (1974). Assessment of depressions: The depression inventory. In Modern Problems in Pharmacopsychiatry, P. Pichot. (Ed). Karger, Bassel: NY, Vol. 7. 3 Spanier, G.B. (1976). Measuring dyadic adjustment: New sclaes for assessing the quality of marriage and similar dyads. Journal of Marriage and Family, 38, 15-28 4 Derogatis, L.R.. Rosen, R. Leiblum, S., Burnette, A. & Heiman, J. (2002). The Female Sexual Distress Scale (FSDS): Initial validation of a standardized scale for the assessment of sexually related personal distress in women. Journal of Sex Marital Therapy, 28, 317-330. * p < .05 Participants’ FSDS total scores significantly decreased post treatment, t(15) = 2.56, p = .05. There were no significant differences found on the BDI or DAS measures post treatment. This study is funded by the BC Medical Services Foundation