Download
1 / 16
160 likes | 312 Views
Describe the clinical features, the genes involved and briefly the testing strategies for familial breast and ovarian cancer. Cancer Genetics Session FRCPath Preparation Course 12/1/10.

E N D
Describe the clinical features, the genes involved and briefly the testing strategies for familial breast and ovarian cancer Cancer Genetics Session FRCPath Preparation Course 12/1/10
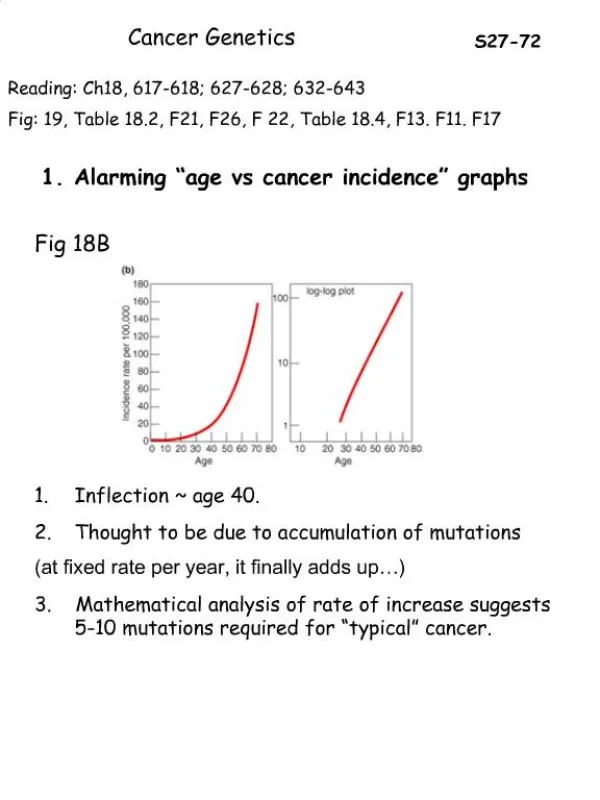
Familial breast cancer accounts for ~5-10% of all breast cancer and familial ovarian cancer accounts for ~8% of all ovarian cancer. • BRCA1 and BRCA2 are the two major genes that confer high risk to both breast and ovarian cancer. • Breast cancer risk is also associated with a number of rare genetic syndromes (<1% of all hereditary breast cancer). • Autosomal Dominant Cancer syndromes: • Li Fraumeni Syndrome (mutations in TP53):Risk of breast cancer 18 fold higher by age of 45yrs. • Cowden Syndrome (mutations in PTEN): Lifetime risk of breast cancer 25-50% with average age of diagnosis 38-46yr. • Peutz-Jeghers Syndrome (mutations in STK11): Risk ~29% by age of 65 years. • Autosomal Recessive syndromes: Breast cancer risk has also been associated in Bloom Syndrome (BLM gene), Werner Syndrome (WRN gene), Xeroderma pigmentosum (8 genes implicated).
Other Genes implicated: • Ataxia telangiectasia/ATM gene: carriers of ATM mutations have a 2-5 fold increase risk of breast cancer. • CHEK2 gene: encodes a cell cycle checkpoint kinase involved in DNA repair. A truncating variant 1100delC estimated to confer a 2fold increase risk of breast cancer in females and 10fold increase risk in males. No increase in risk in carriers of BRCA1/2 mutations. Some evidence suggests a stronger association among families with early-onset breast cancer than those with later-onset breast cancer. • BRCA3: • Linkage to 13q21 in initial study from Scandinavian families negative for BRCA1/2. Not supported by further study of families of Western European ancestry. If a gene does exist it only accounts for a small proportion of non-BRCA1/2 families. • Chromosome 8p also proposed based on studies documenting allelic loss in sporadic cancers. Different LOD scores between studies; If a gene does exist it only accounts for a small proportion of non-BRCA1/2 families. • Low penetrant breast cancer susceptibility genes: • Potential genes involve oncogenes, metabolic pathway genes, oestrogen pathway genes. • Combination of multiple rare or population-specific susceptibility alleles that may confer a low and/or moderate risk – modifying environmental factors.
Clinical features: Predisposition to breast and ovarian cancer BRCA1: Increased risk of colon cancer, pancreatic cancer, gastric cancer, fallopian tube cancer, some association with prostate cancer. BRCA2: Increased risk of male breast cancer, prostate cancer, pancreatic cancer, cancer in bile duct, gall bladder, stomach and melanoma • Tumour characteristics: • BRCA derived breast cancer tumours are overall higher grade compared to sporadic • BRCA1 tumours: more pleiotrophic, higher mitotic count, aneuploid, ER/PR negative, p53 positive, low HER2 expression • BRCA2 tumours: ER/PR positive, p53 positive (may be less than BRCA1), low HER2 expression, similar to sporadic in terms of mitotic rate and pleiotrophism. • Histological and expression differences highlight a different natural history of BRCA1 tumours in relation to BRCA2 and sporadic. • Ovarian tumours are indistinguishable in histology to sporadic. Recent studies attempting to find expression markers for distinction.
Cancer risks/Penetrance: • Breast cancer risk in BRCA1/2 carries has been found to vary by the age at diagnosis and type of cancer in the index case. • Complexity due to environmental and genetic modifiers Based on high risk families Risk of breast cancer by 70yrs: 71% for BRCA1, 84% for BRCA2 Risk of ovarian cancer by 70yrs: 47-63% for BRCA1, 27% for BRCA2 Risk is reduced in estimates based on population based studies: Risk of breast cancer by 70yrs: 65% for BRCA1, 45% for BRCA2 Examples of genetic modifiers: RAD51: A SNP (135G>C) in 5’UTR has been shown to significantly modify breast cancer risk in BRCA2 carriersesp. in homozygotes. SNPs in FGFR2,TNRC9 and MAP3K1 have been associated with increased breast cancer risk inthe general population and BRCA2 carriers (FGFR2 & MAP3K1) and both BRCA1 and BRCA2 carriers (TNRC9).
Ref: Boulton 2006 Biochemical Society Transactions 34, (633–645) BRCA1 Gene • 17q21 • 24 exons (22 coding) • protein 1,863 amino acids – nuclear localisation • exon 11 accounts for ~60% of coding region • genomic region rich in repetitive elements (Alu repeats); promotes instability • Structural motifs: • RING finger domain; cysteine rich domain involved in protein/protein, protein/DNA interaction • - E3 ubiquitin ligase activity. • - Interaction with BARD1 (BRCA1- associated ring domain protein) • - 2 tandem BRCT domains; phospho-serine or threonine binding motif important for protein –protein interaction. Present in various proteins involved in DNA damage response and repair.
Ref: Boulton 2006 Biochemical Society Transactions 34, (633–645) BRCA2 Gene • 13q12 • 27 exons (26 coding) • protein 3,418 amino acids – nuclear localisation • exons 10 & 11 account for ~60% of coding region • Structural motifs: • A transcription activation domain in the N –terminus; possible role in transcription • BRC domain: 70 aa motif repeated 8 times; mediates binding to RAD51. • OB-fold domain: involved in single strand DNA binding • - A RAD51 domain in extreme C-terminus
Functions BRCA1 and BRCA2 implicated in many cellular processes Required for development: embryonic lethality in mice with homozygous deletions of BRCA1/2 Essential role in DNA damage response and maintenance of genome integrity • Tumour suppressor functions: • Tumours in carriers of BRCA1/BRCA2 mutations show LOH of wild type allele • Autosomal dominant mode of inheritance Both genes are expressed in most tissues Precise mechanism of tissue specific tumourigenesis not fully elucidated
BRCA1 cellular functions • DNA damage response and repair • Part of BRCA1 associated genome surveillance complex (BASC)->facilitates • response to DNA repair of DBS by HR and also involved in other pathways (NHEJ,MMR) • Cell cycle checkpoint and apoptosis • Involved in S phase and G2/M checkpoint arrest of the cell cycle in response to DNA • damage. • Transcriptional regulation • Forms complexes with various transcription factors. Implicated in regulation of genes • involved in cell growth, regulation and repair. Role in basal transcription regulation • through interaction with RNA polymerase II • Chromatin remodelling • Interaction with components of the SWI/SNF-related chromatin-remodelling complex. • Ubiquitination • Regulation of proteins involved in DNA repair
BRCA2 cellular functions Involvement in DNA damage repair of DBS by homologous recombination Direct interaction of BRCA2 with RAD51 protein which is essential for DBS by HR. BRCA2 regulates the availability and activity of RAD51, which coats ssDNA to form a nucleoprotein filament that invades and pairs with a homologous DNA duplex to initiate strand exchange in HR BRCA2 contains a region that is capable of inducing transcription and has histone acetylase activity. • Fanconi anaemia/BRCA pathway: • - FANCD1/BRCA2: biallelic mutations cause FA • FA/BRCA pathway involved in DNA repair: FANCD2 protein colocalises with BRCA1 in damaged induced foci. BRCA2/RAD51 also present.
Mutation Spectrum in BRCA1 and BRCA2 • Truncating mutations (nonsense/frameshift/splice site) • Truncating mutations in the central portion of BRCA2 have been associated with increased risk of ovarian cancer and slightly decreased risk of breast cancer • Missense mutations: deleterious when affect highly conserved residues in functional domains • e.g. BRCA1 RING finger missense mutations interfere with BARD1 binding • Complex genomic rearrangements: deletions/duplications. Common ex13 duplication. • Typically arise from unequal homologous recombination mediated by Alu repeats. Also recombination between BRCA1 pseudogene and BRCA1->affecting regulatory sites of promoter. • Account for 5-10% of BRCA1 (depending on population), less for BRCA2. Population Prevalence: Approximately 2% for BRCA1 and BRCA2 from population based case control studies. Increased in families with early onset breast cancer, family history of ovarian cancer and Ashkenazi Jewish ancestry. Founder mutations: Ashkenazi Jewish: BRCA1: 185delAG & 5382insC, BRCA2: 6174delT Icelandic: BRCA2: 999del5 Dutch: BRCA1 large deletions
Mutation Detection • 1) Mutation scanning/Sequencing of variant detected: • -Scanning methods: dHPLC, CSCE, SSCP, DGGE, HRM, PTT • 2) Direct Sequencing: high throughput/automated approach • 3) Mutation specific test: e.g. sequencing, ARMS, taqman etc. • Useful for common founder mutations • 4) Screening for large rearrangements: e.g. QF-PCR, MLPA Exon 11 of BRCA1 and exon 10 & 11 of BRCA2 screened in overlapping fragments due to size. Testing strategy: Testing for founder mutations if case known to be from relevant population Screening for large rearrangements Sequencing of coding exons of both BRCA1/2 in a high throughput manner
Testing considerations: • Interpretation of unclassified variants • Breast cancer is a common disease so phenocopies may exist within families; if there is strong family history and no mutation identified in proband, testing another family member may be considered. • A negative result in BRCA1/2 cannot exclude a heritable predisposition to breast cancer. • Best practice to analyse both genes to completion even if a disease associated mutation has been detected (esp. if carrying out multi-step analysis). • Individuals carrying both BRCA1 and BRCA2 mutations have been reported; especially where there is strong family history on both sides of the pedigree. • In mutation positive cases, ascertainment of which branch of the family mutation is inherited from should take place prior to predictive testing. • Variable penetrance • Negative predictive testing; caution in reducing risk to population; some evidence suggest that risk may still be a little higher than population due to other shared susceptibility genes.
Referral criteria • Typical pattern for BRCA1 and BRCA2 mutation families: • Dominant pattern of inheritance • Multiple cases of breast and ovarian cancer • Young age of onset • Male breast cancer (esp. BRCA2 families) • Bilateral/multiple cancers and tumour phenotype • NICE guidelines (handout): • stratification of women into breast cancer risk categories (population, raised risk, high risk) and guidelines for care, management and surveillance. • Assessment considers family history, cancer types and age at diagnosis of patient and relatives. • High risk: a 10-year risk >8% for women aged 40–49 years or a lifetime risk of 30% or greater, are cared for in tertiary care. High risk also includes a 20% or greater chance of a faulty BRCA1, BRCA2 or TP53 gene in families.
Scottish clinical genetics: Different algorithms to assess score Account for other cancers in the family Combination of NICE and table below used for scoring (aim: mutations detected in 20% of samples tested)
References: Jong et al 2002. Genes other than BRCA1 and BRCA2 involved in breast cancer susceptinility. Journal of Medical Genetics 39:225-242. EMQN best practice guidelines for molecular genetic analysis in hereditary breast/ovarian cancer 2007 Boulton 2006. Cellular functions of the BRCA tumour-suppressor proteins Biochemical Society Transactions 34, (633–645) Mullan et al 2006. The role of BRCA1 in transcriptional regulation and cell cycle control. Oncogene 25, 5854–5863 Gudmundsdottir and Ashworth 2006.The roles of BRCA1 and BRCA2 and associated proteins in the maintenance of genomic stability Oncogene 25, 5864–5874