Download
1 / 25
260 likes | 297 Views
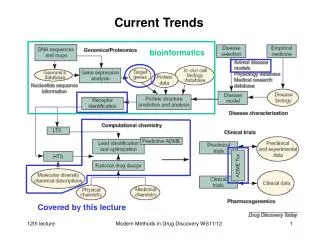
Current Trends in Transplantation. Karin True MD, FASN Assistant Professor UNC Kidney Center May 23, 2011. ESRD Treatment Modalities. Incident patients. Prevalent patients. USRDS 2010 ADR. Incident ESRD patients receiving a transplant within three years of ESRD registration. illi. illi.

E N D
Current Trends inTransplantation Karin True MD, FASN Assistant Professor UNC Kidney Center May 23, 2011
ESRD Treatment Modalities Incident patients Prevalent patients USRDS 2010 ADR
Incident ESRD patients receiving a transplant within three years of ESRD registration illi illi lla lla USRDS 2010 ADR
Advantages of Living Donor • Reduced time to transplant • Fewer deaths awaiting transplant • Pre-emptive transplant possible • Reduced time on dialysis • Hospital stays shorter • Graft and patient survival rates higher
The Living Donor • Free of disease associated with development of kidney dysfunction • Acceptable risk for surgery • Free of diseases which could be transferred to the recipient • Financial gain for the donor is prohibited
Donor Outcomes • Survival similar to matched controls • ESRD in 11 donors • 180 per million/yr • In general population • 286 per million/yr NEJM 2009; 360: 459-469
Donor Outcomes cont. Donors perception of benefit to recipient Quality of life scores AJT 2011; 11:463-469
Laprascopic Donor Nephrectomy • Advantages • Pain control • Decreased hospital stay • Earlier return to ADLs • Better wound cosmesis • Disadvantages • Increased warm ischemia time • Smaller surgical field • Hand assisted technique may aid in hemorrhage control • Difficult in obese donors Br J Surg 2010; 97: 21-28
Living Donor Relationships USRDS 2010 ADR
HLA Matching • The Major Histocompatibility Complex (MHC) is a large cluster of closely linked genes on the short arm of chromosome 6 • These genes code for a group of proteins called the Human Leukocyte Antigens (HLA) • determine the rejection or acceptance of tissue grafts • involved in antigen presentation • markers of cellular identity, self-recognition • Transplant focuses on HLA –A, -B and –DR • specific HLA alleles are numbered • one from each parent • Ex. of HLA type: A1 A2 B51 B60 DR7 DR11
Crossmatch A2 IgG to A2 A2 IgG to A2 A2 Positive Crossmatch Predicts rejection Negative Crossmatch Proceed with transplant
Blood Type Compatibility Median wait time for a deceased donor 5.1 years 3.3 years 5.3 years 2.3 years 30-35% chance a given pair will be ABO incompatible
Paired Donation Recipient A Donor A X Transplants done with a negative crossmatch Donor B Recipient B X
Disadvantages • Pairs with type O recipients less likely to match • Type O donors usually compatible • Match rates only ~15% • ~50% for those with non-type O recipients • Ideally surgeries occur simultaneously • Donors have autonomy to withdraw consent • Not always possible with bigger chains • Geographic barriers • May separate donor from recipient at time of surgery • Lack of national registry • Need maximum number of pairs for success
ABO Incompatible Transplant • Use isohemaglutinin techniques to measure titers of anti-A and anti-B antibodies present • Need to eliminate these antibodies to have a successful transplant • Strategies • Therapeutic plasma exchange • centrifuge separation of plasma w/ removal of immunoglobulin, complement, clotting factors • can run concurrent with hemodialysis • IVIG • downregulates antibody production • usually used as an adjunct to plasma exchange • Once titer is low enough (center specific) can proceed with transplant
Disadvantages • Antibody mediated rejection • 10-30% early • 0-10% irreversible leading to graft loss • > 1 month survival similar to routine transplants • Cost from POD -14 to +90 • ABOI: $90,300 + 68,100 • ABOC: $52,500 + 25,300 • Differential $37,800 • Less than the cost of a year of hemodialysis Curr Op Tx 2010; 15:526-530 • Transplantation 2006; 82:155-163
Desensitization • Therapies to reduce/eliminate the HLA antibodies the recipient has to the donor • Done prior to transplant over a period of weeks to months • Treatment options • Plasmapheresis • IVIG • Rituximab • Other – bortezemib, eculizumab, splenectomy
Desensitization • Outcomes • At 2 years • Patient survival 95% • Graft survival 86% • Decreased compared to traditional transplants • Consider paired donation first • Disadvantages • Rejection • 36% acute rejection (28% antibody mediated) • Higher rate of transplant glomerulopathy • Once develops is poor prognosis • More immunosuppression • Cost CJASN 2011; 6:922-936
ECD and DCD Donation Incidence of delayed graft function (DGF) USRDS 2010 ADR
Patient survival Graft survival
Medicare Costs by Modality USRDS 2010 ADR