Download
1 / 67
880 likes | 1.63k Views
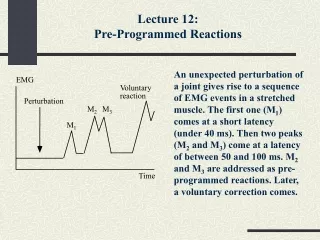
Jose Paciano Reyes, MD, FPNA ASMPH. Introduction to EEG, EMG-NCV. E lectro E ncephalo G raphy. What is EEG?. Non-invasive recording of brain electrical activity from electrodes placed on the scalp. Uses of EEG in epilepsy. Evaluation of suspected epilepsy

E N D
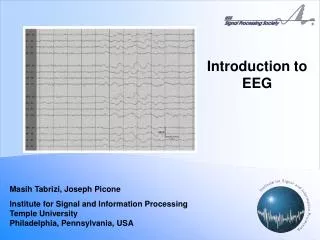
Jose Paciano Reyes, MD, FPNA ASMPH Introduction to EEG, EMG-NCV
What is EEG? • Non-invasive recording of brain electrical activity from electrodes placed on the scalp
Uses of EEG in epilepsy • Evaluation of suspected epilepsy • Presence of electrographic seizure activity during a behavioral disturbance that could represent a seizure establishes the diagnosis • May detect interictal epileptiform activity • Classification of seizure disorder • Petit mal: episodic generalized 3 Hz spike-and-wave activity • Complex partial seizures: focal epileptiform discharges
Uses of EEG in epilepsy • Assessment & prognosis of seizures • Normal EEG implies a more favorable prognosis for seizure control • Management of status epilepticus • Monitor seizure activity in patients who have received neuromuscular blocking agent or on pentobarbital-induced coma • Diagnosis of non-convulsive status epilepticus or absence status epilepticus
Other uses of EEG • Detection of structural brain lesions • Diagnosis of neurologic disorders • Herpes simplex encephalitis – repetitive slow wave complexes over temporal lobes • Creutzfeldt-Jakob disease or SSEP – periodic complexes in a patient with an acute dementing disorder • Evaluation of altered consciousness
How does it work? • Sum of excitatory postsynaptic potentials (EPSPs) & inhibitory postsynaptic potentials (IPSPs) • EEG rhythm depends on thalamic pacemaker cells and the reticular activating formation • 1/3 of the cortex can be seen by scalp electrodes • At least 6 cm2 of cortex must be involved to be detected by surface electrodes
Excitatory Synaptic Potentials &Spike Generation 0 E mV E Threshold -60 Resting potential EPSP -70 Time
Interaction of Excitatory & Inhibitory Synapses 0 E I E mV Threshold -60 -70 Time IPSP
The main generators of the EEG are voltage gradients along dendrites in the upper cortical layers. This in turn causes a current flow in the conducting medium surrounding it. Several thousands of parallely oriented neighboring dendrites have to be active synchronously to produce a measurable signal. • The summed activity within a small area of cortex can be described by a so-called “dipole”.
How is it done? 10-20 System
How is it done? • Montages • Bipolar • Localizes potential by direction of pen deflection (phase reversal) • Distorts shape and amplitude • Referential • Localizes potential by amplitude of pen deflection • Potentials at the reference electrode may appear in all channels • Interelectrode distance alters amplitude
How is it done? • Activation procedures • Hyperventilation • Normal: generalized slowing (3 – 5 min) • Elicits 75% of absence seizures • Photic stimulation • Normal: occipital driving at stimulus frequency or no response • Photoconvulsive response
Frequency Generalized asynchronous slow waves (anoxia) Focal slow wave(stroke, tumors, multiple sclerosis) Epileptiform discharge Spikes Sharp waves EEG abnormalities • Amplitude • Decreased generalized activity (hypoxia, hypothermia) • Decreased alpha (mild metabolic disturbances) • Decreased focal activity (stroke, tumors) • Increased beta (hyperthyroidism, benzodiazepines)
Choline Acetate Presynaptic receptors Choline Na+ Achesterase A AcCoA + Choline ChAT B Ach ATP, P Ach ATP, P ACh ACh Axon Nicotinic Receptors Ca2+ Nerve terminal Muscle
What is EMG-NCV? • Technique in the diagnosis of myopathic and neurogenic disorders • Assessment of neuromuscular transmission • Assessment of peripheral nerve and root disorders (diffuse neuropathy, focal lesion, evaluate severity of nerve injury) • An extension of the neurologic examination
Uses of Nerve Stimulation Studies • Determine whether sensory symptoms are caused by a lesion proximal or distal to the dorsal root ganglion • Detecting subclinical involvement of other perpipheral nerves • Determine site of a focal lesion and prognosis • Distinguish between polyneuropaty and mononeuropathy multiplex • Follow progression of peripheral nerve disorders • Indicate predominant pathologic change demyelinating vs axonal neuropathies
Uses of Electromyography • Detect disorders of the motor units and can indicate the site of the underlying lesion (anterior horn cell, spinal root, plexus, peripheral nerve) • Recognition of neuromuscular disorders • Provide a guide for prognosis
How is it done? • Motor Nerve Conduction Studies • Recording the electrical response of a muscle to stimulation of its motor nerve at two or more points along its course. • Compound muscle action potential Latency, amplitude, nerve conduction velocity
How is it done? • Sensory Nerve Conduction Studies • Recording the electrical response of a sensory nerve to stimulation at one or more points along its course. • Sensory nerve action potential Latency, amplitude, nerve conduction velocity Orthodromic, Antidromic
How is it done? 1st amplitude 2nd amplitude MV or uV 1st latency 0 2nd latency 0 msec
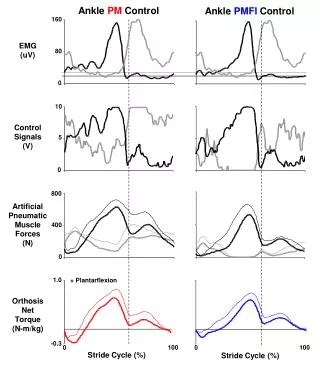
H-reflex Neurophysiologic counterpart of the ankle jerk Seen only calf muscles in adults Submaximal stimulus Stimulate IA afferent sensory nerve Involves a synapse Represents nerve conduction velocity near cord Faster than F-waves Nerve Conduction Studies • F-wave • Measure in any motor nerve • Supramaximal stimulus • Antidromic conduction, measure reflected impulse • No synapse • Tests entire length of motor nerve • Slower than H-reflex • Very early finding in GBS
How is it done? • Electromyography - Activity at Rest • Insertional Activity • Crisp burst of activity as needle enters • Increase with denervation or irritation • Decreased when muscle is replace by fat or connective tissue Fibrillation potentials positive sharp waves • Muscle fiber irritability Fasciculation potentials • Spontaneous activity of motor units
How is it done? • Electromyography - Activity During Voluntary Muscle Contraction • Motor Unit Potentials • Recorded with minimal muscle contraction • Amplitude (0.5 – 5.0 mV) decreased in myopathy and increased with reinervation and axonal sprouting • Duration (5 – 14 msec) decreased in myopathy and increased with renervation • Polyphasic in myopathy and renervation
How is it done? • Electromyography - Activity During Voluntary Muscle Contraction • Interference Pattern • Recorded during maximal muscle contraction • Decreased recruitment seen in neuropathic process • Increased recruitment seen in myopathic process
Electromyography • Endplate activity • Normal spontaneous finding near endplate • Ocean surf sound • Fibrillations • Positive sharp waves • Nerve potentials
Electromyography • Positive Sharp Waves • Monophasic downward (positive) deflection • Dull thuds, like rain on tin roof • Duration: 4 – 20 msec • Amplitude: 50 - 4000 mV • Indicate denervation or myopathy
Electromyography • Fibrillation • Spontaneous firing of single muscle fiber • Diphasic with initial downward (positive) deflection • Sounds like crisp tics • Duration: 0.5 – 3 msec • Amplitude: 50 - 200 mV • Indicate hypersensitivity of muscle to Ach or axonal injury or myopathy • 10% of normal muscles have areas of fibs
Electromyography • Fasciculation • Spontaneous firing of single motor unit action potential • Large deflections • Usually occur with proximal lesions like those of the nerve root or anterior horn cells • Occur in 15% of normal population
Electromyography • Myotonic Potentials • Spontaneous discharges that wax and wane in frequency and amplitude • Dive bomber sound • Indicate myotonic disorders and periodic paralysis • Resolve in true myotonia
Electromyography • Giant MUAPs • MUAP > 5 mV during active contraction • Indicate renervation with axonal sprouting and chronic changes
Electromyography Myopathic pattern • Chronic • Decreased CMAP amplitude • Decreased insertional activity • No fibrillations or postive sharp waves • Active • Small, short duration CMAP • Increased recruitment • Decreased interference pattern amplitude • Fibrillations • Positive sharp waves
Axonal Degeneration vs. Segmental Demyelination: Electrophysiologic Features • Axonal Degeneration Segmental Demyelination • Motor Nerve Conduction Studies • CMAP amplitude Decreased Normal (except with CB) • Distal latency Normal Prolonged • Conduction velocity Normal Slow • Conduction block Absent Present • Temporal dispersion Absent Present • F wave Normal Prolonged or Absent • H reflex Normal Prolonged or Absent
Axonal Degeneration vs. Segmental Demyelination: Electrophysiologic Features • Axonal Degeneration Segmental Demyelination • Sensory Nerve Conduction Studies • SNAP Amplitude Decreased Normal • Distal latency Normal Prolonged • Conduction Velocity Normal Slow Needle EMG Spontaneous Activity • Fibrillations Present Absent • Fasciculations Present Absent Voluntary Motor Unit Potentials • Recruitment Decreased Decreased • Morphology Long duration/polyphasic Normal
NCV FACTS • Reinervation begins 1-3 weeks after injury, progress at 1 mm/day and EMG evidence is not seen for weeks or months • After trauma, neuromuscular transmission fails before NCV change • Sensory NCV preserved > motor NCV