Download
1 / 43
430 likes | 556 Views
Health-related Fitness Components. Dr. Suzan Ayers HPER Dept Western Michigan University. Fitness Components. Cardiovascular endurance Muscular strength/endurance Flexibility Body composition/Nutrition. Aerobic Fitness. Based on:

E N D
Health-related Fitness Components Dr. Suzan Ayers HPER Dept Western Michigan University
Fitness Components • Cardiovascular endurance • Muscular strength/endurance • Flexibility • Body composition/Nutrition
Aerobic Fitness Based on: Franks, B.D. (1999). Personalizing Physical Activity Prescription. Scottsdale, AZ: Holcomb Hathaway Publishers.
Components of Cardiovascular Training Session • Warm-up prior to physical activity • Prepare heart & other muscles for more intense activity • Raise core body temperature • Physical activity participation • Principles of Fitness (FITT) • Frequency • Intensity • Time (duration) • Type (mode) • Overload (more than normal) • Progression (using FITT to increase overload) • Cool-down after physical activity
Related Terminology (Howley & Franks, 1997) • Cardio: heart • Vascular: blood vessels • Respiratory: lungs and ventilation • Aerobic: working with oxygen
Structure/Function of the CV System • Heart: Fist-sized • Blood Flow: RAV Lungs LAV Aorta Body • Function: • Systole (contraction) • Diastole (rest) • Blood pressure (sbp/dbp) • Factors influencing HR: • Body position -Temperature • Fitness -Stimulants • Age -Depressants • Gender • Mood
Benefits of Participation in Cardiovascular Activities • Psychological Health • Stress management • Reduced nervous tension • Increased Cardiovascular System Efficiency • Control of various chronic degenerative diseases: • Adult-onset diabetes • Asthma • Hypertension • Obesity • CVD
Measuring Heart Rate • Why? • To optimize health benefits • To assess student EFFORT • Where? • Radial (below thumb) • Carotid (on neck) • How? • Palpate for: 60s, 30s x 2, 15s x 4, 10s x 6, 6s + 0 • HR monitor • Cautions: • Never use thumb to palpate • Count 0, 1, 2, 3, etc. • Higher HR greater measurement error
Determining HR Zones • Max HR (MHR): 220-age • Resting HR (RHR): • Awaken & check before lifting head; repeat for 6 days and average • In school setting: lay down on floor for 10 mins then check • Target Heart Rate Zones (THRZ): • 50-60%MHR: sufficiently strenuous daily PA • 60-70%MHR: fat burning • 70-80%MHR: improved CV endurance • 80-100%MHR: competitive training • Recovery Heart Rate: • How long it takes the heart to return to “normal” after PA • Usually one, three, five minute intervals
Karvonen Formula • More precise for very fit or unfit students • 220-age = MHR • MHR-RHR = HRR (reserve) • HRR * lower %MHR = low1 • Low1+RHR = lower limit of THRZ • HRR*upper %MHR = up1 • Up1+RHR = upper limit of THRZ Karvonen Formula: 220-35=185–50=135 135 x 0.7x .85 95 115 +50+50 145 165 General Formula: 220-35=185 185 x 0.7x .85 130 157
Age and grade-based Heart Rate Training Zones Age Grade Max HR (MHR) 220-age Target Heart Rate Zone (THRZ) 70-85% General Ranges 6 K 214 150-182 Elementary: 150-195 7 1 213 149-181 8 2 212 148-180 9 3 211 148-179 10 4 210 147-179 11 5 209 146-178 12 6 208 146-177 Middle: 140-180 13 7 207 145-176 14 8 206 144-175 15 9 205 144-174 High: 140-165 16 10 204 143-173 17 11 203 142-173 18 12 202 141-172
Age Max HR (MHR) 220-age Target Heart Rate Zone (THRZ) 60-75% Physical Best Age-based Heart Rate Training Zones 6 214 128-161 7 213 128-160 8 212 127-159 9 211 127-158 10 210 126-158 11 209 125-157 12 208 125-156 13 207 124-155 14 206 124-155 15 205 123-154 16 204 122-153 17 203 122-152 18 202 121-152
Developmentally Appropriate Guidelines • Table 6.2 (p. 89): • Primary Ss (K-2): Introduce concept of feeling heart rate and noticing changes with activity levels • 4th-5th grade Ss: use carotid artery & wrist to count pulse, calculate MHR & THRZ • MHR and THRZ (60-75% MHR) • Table 6.4 (p. 91): • Primary Ss (K-2): 3-5 minutes • Intermediate (3-5): 10 minutes • MS/HS: 20+ minutes
Personalized Physical Activity Recommendations • Model for Making Personalized Physical Activity Recommendations (Franks, 1999): Level 1: Activities for Everyone Level 2: Activities for Sedentary People Level 3: Activities for Moderately Active People (Health) Level 4: Activities for Moderately Active People (Fitness) Level 5: Activities for Vigorously Active People (Performance) LPAM EPM
Activities for Everyone • “Activities for everyone should be of the type that can be done as part of an individual’s routines at home, work, and during leisure time” (Franks, 1999). • Walk or ride your bike to school rather than take the bus • Climb stairs rather than using the elevator • Park farther away from the store and walk • Perform daily stretching to prevent low back problems
Activities for Sedentary People • Sedentary: Cannot walk for 30 minutes continuously without discomfort or pain • “Inactive individuals should continue to find ways to include activity in their daily routineand should accumulate at least 30 minutes of moderate-intensity activity daily” (Franks, 1999). • Walking, yard work, cycling, slow dancing, low-impact aerobics • Physical activity periods broken into 2-4 segments daily • Emphasis on the accumulation of daily physical activity rather than intensity
Activities for Moderately Active People With Health Goals • Moderately active: Accumulate 30 minutes of activity daily, or who can walk 30 minutes continuously without pain or discomfort, but could not jog 3 miles (or walk 6 miles at a brisk pace, cycle 12 miles or swim ¾ mile) continuously without discomfort and undue fatigue • Individuals with specific health goals should perform the following activities (Franks, 1999): • Cardiovascular • Accumulate at least 30 minutes of moderate-intensity activity • Include longer duration and/or higher intensity
Activities for Moderately Active People With Fitness Goals • Individuals with specific fitness goals should perform the following activities (Franks, 1999): • Aerobic Fitness • 20-40 minutes of vigorous-intensity activity, 3-5 days/week • THRZ 70-85% for adults • Fast walking, jogging, cycling, fast dancing, low- to moderate-impact exercise to music, swimming
Activities for Vigorously Active People With Performance Goals • Vigorously active: Can run 3 miles continuously (or walk fast 6 miles, cycle 12 miles or swim ¾ mile) within the THRZ 3-4 times a week without discomfort or pain • Individuals who are vigorously active and who have specific performance goals should perform the following activities (Franks, 1999): • Sport or Physical Task(s) • Develop and/or maintain fitness levels • Interval training • Motor tasks related to performance • Specific skills related to performance • Strategy and mental readiness
Muscular Fitness Lecture based on the work of Roberts, S.O. (1996). Developing Strength in Children: A Comprehensive Guide. Reston, VA: AAHPERD Publications.
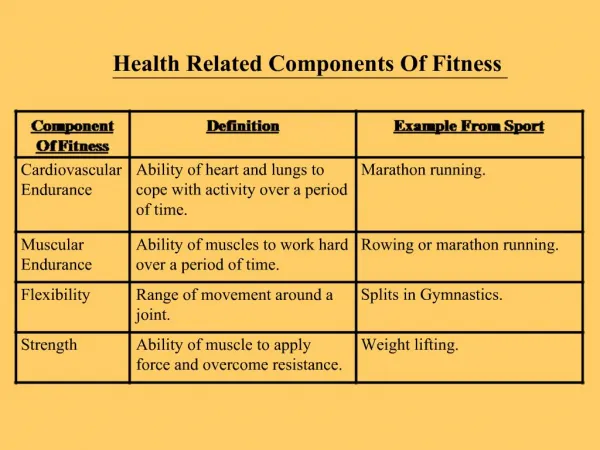
Muscular Strength andEndurance Defined • Muscular strength • “The ability of a muscle or group of muscles to exert maximal force against a resistance” (AAHPERD, 1999) • One repetition maximum (1RM) • Muscular endurance • “The ability of a muscle or muscle group to exert force over a period of time against a resistance less than the maximum an individual can move” (AAHPERD, 1999) • Submaximal muscle contractions over a high number of repetitions with little rest/recovery • Often difficult to separate the two in physical education
Major Controversies Related to Youth Strength Training (Roberts, 1996) • Myth 1: Children are not able to develop strength beyond that generally associated with normal growth and development • Myth 2: Children should not lift weights or participate in resistance training programs because of the risk of injury to the epiphyseal plates • Myth 3: There is not enough evidence to support a structured resistance training program for children
Factors Influencing Children’s Strength Development(Kramer, Fry, Frykman, Conroy & Hoffman, 1996) • Hormonal Influence • Increase in circulating androgens • Increase in lean body mass • Neurological Influence • Increased motor unit activation • Neural myelination development • Fiber Type Differentiation • Significant increase in muscle fiber size
Injuries Related to Children’s Participation in Strength Training • Historical Perspective • Growth plate injuries in adolescent children following strength training (Gumps, Segal, Halligan, & Lower, 1982; Risser, Risser, & Preston, 1990; Ryan & Salciccioli, 1976). • Recommendation that children avoid formal strength training • Contemporary Perspective • More recent studies have suggested strength training is safe in properly supervised programs (Ramsay, Blimkie, Smith, Garner, Macdougall, & Sale, 1990; Weltman, Janney, Rians, Strand, Berg, Tippet, Wise, Cahill, & Katch, 1986). • Serious injuries related to “excessive” overhead lifts & improper supervision
Health-Related Benefits Prevention of CVD Reduction and control of obesity & hypertension Improved self-confidence & self-image Development of good posture Improved body comp Improved flexibility Establishment of lifetime interest in fitness Benefits of Strength Training • Skill-Related Benefits • Improved ability to perform basic motor skills • Possible prevention of injuries • Greater ease & efficiency of sport skill performance • Early development of coordination & balance • Better performance on nationwide fitness tests
Professional Guidelines & Recommendations • Professional position statements on youth strength training (ACSM, 1988; AAP, 1983, 1990; NSCA, 1985, 1996). • Proper supervision & technique instruction are critical • Focus on technique development & affective domain • Emphasize a variety of activities & skill development • Avoid the use of maximal lifts with children & adolescents • Sample training protocol: • Initial focus on lifting technique • High reps & light weight • 1-3 sets x 6-15 reps • 8-10 different exercises • 2-3 nonconsecutive days per week
Flexibility Defined • Flexibility • “The range of motion (ROM) available in a joint or group of joints” (Alter, 1996) • Types of stretching • Static: using the ROM of a joint slowly & steadily in a held position • Dynamic: moving in a ROM necessary for a sport • Ballistic: quickly and briefly bouncing, rebounding or using rhythmic motion in a joint’s ROM (mimics sport movements) • PNF (proprioceptive neuromuscular facilitation): using the body’s reflexes to relax a muscle before stretching it • Laxity • “The degree of abnormal motion of a given joint” (Alter, 1996) • Also referred to as “double-jointedness”
Teaching and Training Guidelines for Flexibility • Teaching • Never make stretching competitive • Emphasize correct technique and personal bests • Training principles • Intensity: How the stretch feels • Time: Length of stretch x number of time each stretch is done • Type: Specific muscles stretched • A static stretch beyond the point of mild discomfort to pain merely increases the likelihood of injury
Stretching Controversies(Alter, 1996) • Static • Most appropriate for physical education • Proven effectiveness • Ease of implementation • Ballistic (dynamic, fast, isotonic, kinetic) • Often maligned as dangerous • Develops dynamic flexibility • Generally more interesting • Inadequate time for tissues to adapt to the movement • Increased likelihood of soreness • Inadequate time for neurological adaptation to the movements
Factors Limiting Flexibility(Alter, 1996) • Connective tissues in joints/muscles lacking elasticity • Muscle tension • Poor coordination and strength during active movements • Limitations caused by bone & joint structures • Pain
Professional Guidelines & Recommendations • Warm-up with whole-body activity first • Use slow, controlled movements • Hold each stretch 10-15, 15-30, OR 30-60 seconds • Encourage individualization • Excess body fat does NOT impede flexibility • More flexible groups: • Females • Individuals under 6 and between 12 and young adulthood
Body Composition & Nutrition Lecture based on the work of Wilmore, J.H. (1999). Exercise, Obesity, and Weight Control. Scottsdale, AZ: Holcomb Hathaway, Publishers.
Overweight & Obesity Defined • Overweight • “Body weight that exceeds the normal or standard weight for a particular person, based on his or her height and frame size.” • Measured with height/weight tables. • Over the 85th percentile • Obesity • “Condition in which the individual has an excessive amount of body fat” • Males over 25% & women over 35% body fat are obese • Males 20-25% & women 30-35% body fat are considered to have borderline obesity • Over the 95th percentile • Variety of laboratory & field assessment techniques used to measure a person’s body composition: • Hydrostatic weighing • Bioelectrical impedance • Ultrasound • Skinfold
Body Composition Values Interesting links: http://www.am-i-fat.com/body_fat_percentage.html http://www.am-i-fat.com/body_mass_index.html http://team.liu.edu/~/~Lopos/fp/bodyc.htm http://www.christie.ab.ca/aadac/WhoAmI/perfectbody.htm
Prevalence of Obesity in the U.S. • Dramatically increasing trend in the prevalence of obesity over the past 30 years in the U.S. • National Center for Health (1986): • 28.4% of American adults aged 25-74 years are overweight. • Between 13% and 26% of U.S. adolescent population are obese with an addition 4% to 12% being super-obese, depending on gender and race. • These figures represent a 39% increase in the prevalence of obesity when compared with data collected in 1966 and 1970. • Gortmaker, Dietz, Sobol, & Wehler (1987): • Reported 54% increase in prevalence of obesity among children aged 6 to 11 years.
Health Implications of Obesity • Medical Risks • Increased risk for general excess mortality. Possible causes include heart disease, hypertension, & diabetes. • Upper body obesity (“apple-shaped”) involves increased risk of cardiovascular disease, hypertension, stroke, elevated blood lipids, and diabetes. • “Pear-shaped” individuals have excess weight on the hips and thighs (less cardiovascular risk). • Low Physical Fitness Levels • Psychosocial Effects
Physiological Considerations • The Control of Body Weight • Balance between caloric intake & expenditure. • Etiology of Obesity • Complex and multi-factored: • Genetic influences • Hormonal imbalances • Alterations in homeostatic function • Physiological & psychological trauma • Emotional trauma • Environmental factors • Cultural habits • Inadequate physical activity • Improper diet
Weight Reduction and Control • Behavior Modification • Dietary intake • Physical activity • Body Composition Myths • Fad diets • Spot reduction • Low intensity versus high intensity aerobic exercise • Exercise devices for fat reduction
Diet and Nutrition • Diet: • Total calories consumed in 5-7 day period • “Good” nutrition • Variety of foods • Provides adequate nutrients • Supplies sufficient energy to maintain ideal body mass • Agencies developing guidelines: • Committee on Dietary Allowances: RDAs • Food and Drug Administration • USDA: Food Guide Pyramid • Adolescent nutritional needs (Saltman, Gurin & Mothner, 1993): • Females: 2,200 cals/day • Males: 3,000 cals/day
Consequences of an Unhealthy Diet • Increased calories consumed by eating “low cal” foods • High protein/low carbohydrate diets suppress appetite; can be toxic over time • High carbohydrate diets can compromise energy intake and provide too little protein • Over-consumption of vitamins/minerals only generates expensive urine • Good diet NOR physical activity alone can = fitness
Harvard School of Public Health (2004) http://www.hsph.harvard.edu/nutritionsource/pyramids.html