Download
1 / 15
150 likes | 546 Views
Background. Big change in recent years in care of people with acute ischaemic stroke

E N D
1. Diagnosis and management of TIA and ischaemic stroke in the acute phase BMJ 2011
McArthur et al.
University of Glasgow
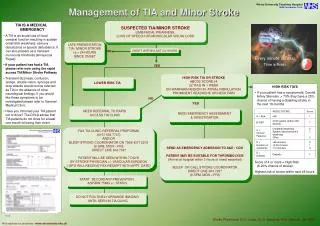
2. Background Big change in recent years in care of people with acute ischaemic stroke � both stroke and TIA now recognised as medical emergencies that should be treated as urgently as MI.
Thrombolysis widely adopted
�Cautious optimism has replaced therapeutic nihilism� but still an important cause of death and disability
An estimated 900,000 stroke survivors in England, half of whom dependent on others for care (estimated cost �8bn per year). Number likely to increase as demographics change
3. Terminology, classification Stroke (cerebrovascular event, brain attack) still classified as haemorrhagic or ischaemic
TIA � similar symptoms but last less than 24 hours, but truly �transient� attack, with no cerebral infarction, only minutes; longer attacks probably should be considered as stroke, and terminology likely to change in the future
Oxford classification �
TACS, PACS, LACS, POCS
Once confirmed as ischaemic, terminology changes to e.g. PACI (Partial anterior circulation infarct).
4. Pathological process Sources of cardiac emboli � AF, mural thrombus, valve disease large intracerebral arteries (e.g. MCA)
Atherosclerotic disease typically affects the extracranial internal carotid artery, also vertebral and basilar arteries
Lacunar infarction � from occlusion of deep perforating arteries (both anterior and posterior circulation) white matter of cerebral hemispheres and brainstem
5. Oxford system of stroke classification Total anterior circulation stroke (TACS)
All three of:
� Contralateral motor or sensory deficit
� Homonymous hemianopia
� Higher cortical dysfunction* Posterior circulation stroke (POCS)
Any one of:
� Isolated homonymous hemianopia
� Brain stem signs
� Cerebellar ataxia
6. Is it a stroke? One study of 350 admissions for suspected stroke � 30% had non-stroke diagnosis
Tools do help diagnosis �
FAST (Face Arm Speech Test) � PPV of 78%
ROSIER scale � similar Frequency of common conditions that mimic stroke
Seizure 21%
Sepsis 13%
Toxic/metabolic 11%
Space occupying lesion 9%
Syncope 9%
Delirium 7%
Vestibular 7%
Mononeuropathy 6%
Functional 6%
Dementia 4%
Migraine 3%
Spinal cord lesion 3%
Other 3%
7. Imaging Non-contrast CT � still widely used � useful for excluding haemorrhage and SOL
�but...detection of ischaemia is poor in very early stages
Differentiating ischaemia from haemorrhage can be difficult after several days
MRI � preferable � much better sensitivity in detection of early ischaemia (83% vs CT 26%)
8. TIA If ongoing symptoms (even if only mild), treat as possible stroke and admit urgently
Overall 7 day risk of stroke = 5.2% (recent systematic review)
ABCD2 estimates risk of recurrence at 2 days - useful in risk stratification and in diagnosis � many centres offer same day appts for those at highest risk � this should probably be the aim for all patients with TIA
NICE & SIGN guidelines recommend aspirin 300mg and urgent referral, with ABCD2 score >4 seen within 24 hrs
EXPRESS study got TIA patients seen in Oxford with �immediate access� � achieved 80% reduction in recurrent stroke at 90 days (if replicated could mean 10,000 stroke events prevented annually).
9. What will specialist centres do? Confirmation of stroke diagnosis
Identification of causes
Timely initiation of evidence based treatment
TIA
Ischaemic stroke
Aspirin
Thombolysis
Surgical intervention
10. Patients with TIA Treatments are aimed at preventing a further event
Confirmed atrial fibrillation or mural thrombus
anticoagulants
All patients ->
antiplatelet or anticoagulant drugs
lipid lowering therapy
antihypertensive therapy
carotid surgery,
treatment of diabetes
advice about diet, lifestyle, and smoking cessation.
A recent focus of research has been the potential benefits of early antiplatelets, statins, and antihypertensives (results of EXPRESS may be down to this).
�acute� prescription of antihypertensives may have no clinical benefit, although results from current studies awaited.
11. Patients with acute ischaemic stroke - Aspirin for every 1000 patients treated acutely with aspirin (160-300 mg) 13 fewer deaths occurred by the end of follow-up - systematic review of antiplatelets after ischaemic stroke (n=43041)
UK guidelines recommend that patients with acute ischaemic stroke are prescribed aspirin 300 mg daily for two weeks, followed by a long term secondary preventative antiplatelet strategy.
Aspirin should be withheld for 24 hours after thrombolysis.
rectal preparations may be used is swallowing a problem.
Use clopidogrel if patients unable to take aspirin
no evidence to support early anticoagulation as a treatment for acute ischaemic stroke.
12. Patients with acute ischaemic stroke � benefits of early thrombolysis Alteplase (rt-PA) is beneficial if given within 4.5 hours of acute ischaemic stroke.
Reduces longer term disability but not improved survival or immediate neurological improvement
Two recent pooled meta-analyses of the major thrombolysis trials (n=277521 and n=367022) demonstrated early thrombolysis -> clear benefit with significantly better outcomes. In the larger analysis the odds ratios of a favourable outcome with rt-PA were
2.55 (95% CI 1.44 to 4.52) for 0-90 minutes,
1.64 (1.12 to 2.4) for 91-180 minutes,
1.34 (1.06 to 1.68) for 181-270 minutes,
1.22 (0.92 to 1.61) for 271-360 minutes
Trials have reported that mortality rates at three months are equivalent to placebo.
13. Patients with acute ischaemic stroke � problems with early thrombolysis Limited time window is a major barrier to its delivery.
The risk:benefit ratio beyond 4.5 hours has not been fully established and ongoing clinical trials aim to provide further evidence.
Patients older than 80 years were excluded from most of the clinical trials. Observational data suggest that their risk:benefit ratio is similar to that of other patients
Risk of iatrogenic intracerebral haemorrhage after thrombolysis - patient selection guidance is designed to minimise this risk.
Contraindications to thrombolysis an evolving landscape, so refer anyway
Provision of a comprehensive thrombolysis service demands substantial economic investment and infrastructural change � still considerable geographical disparity in availability and use of rt-PA
14. Patients with acute ischaemic stroke � surgical intervention �Malignant� swelling of an infarcted cerebral hemisphere can occur in first few days esp following TACI/PACI
uncommon
associated with a very high mortality.
surgical intervention saves lives and reduces disability in selected patients <60.
meta-analysis of three RCTs - surgical craniotomy NNT=2 to reduce disability.
But�reducing mortality at the expense of substantial disability remains a possibility � accurate selection of patients is vital, more research needed.
15. Key messages Education of patients and their relatives to recognise signs of stroke and transient ischaemic attack (TIA) is crucial to promote early presentation to medical services
TIA and stroke are medical emergencies; refer for urgent specialist opinion
Eligibility for acute treatments is constantly evolving, discuss any patient with possible acute stroke with the local stroke team
The risk of further cerebrovascular event following TIA is substantial, immediate, quantifiable, and preventable; do not be reassured by resolution of symptoms
Effective treatments for selected stroke patients include: aspirin within first 48 hours; intravenous thrombolysis; surgical decompression of cerebral oedema
A sudden change in consciousness of an acute stroke patient may indicate a treatable complication and warrants urgent investigation
Admission to a dedicated stroke unit offers mortality and functional benefits to all patients with stroke
16. So...does this review help us? What was new to you?
In what areas do you need to change your approach or your practice?
What are you going to share with your colleagues back at the surgery?