Download
1 / 22
250 likes | 1.01k Views
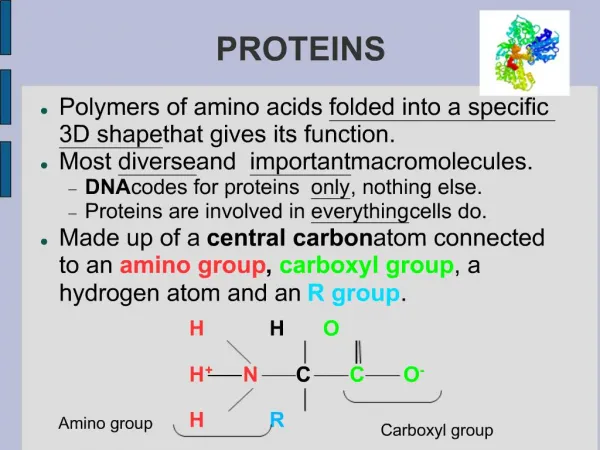
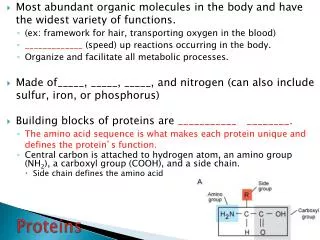
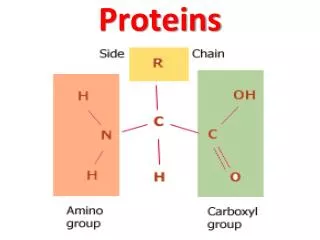
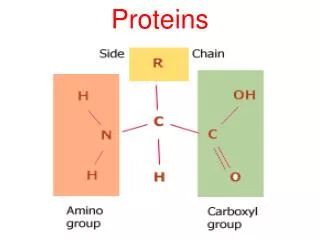
Proteins. OVERVIEW. 1.Physiological characteristics 2. Measurement: serum protein and electrophoresis 3. Serum protein abnormalities 4. Fibrinogen. Physiological Characteristics. Proteins.

E N D
OVERVIEW 1.Physiological characteristics 2. Measurement: serum protein and electrophoresis 3. Serum protein abnormalities 4. Fibrinogen
Proteins -Fresh serum contains all plasma proteins except those consumed during clot formation (fibrinogen and factors V+ VIII) -Total proteins comprise ALBUMIN and GLOBULINS ALBUMIN is synthesised by the liver GLOBULINS are mainly synthesised by B-Lymphocytes and the liver: & fractions and fractions N.B. There is one albumin (relative molecular weight of 66) and thousands of globulins (with higher relative molecular weight, i.e. IgG=150)
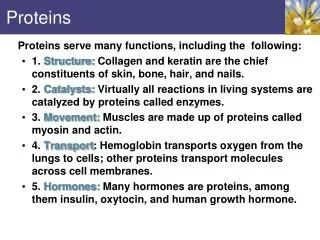
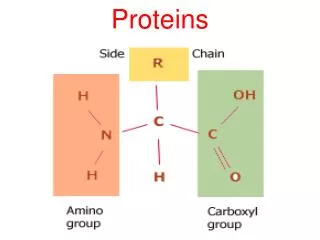
-Maintenance of oncotic pressure (esp. albumin) -Buffering capacity (esp albumin) -Transport of molecules (e.g. drugs, lipids, hormones, metals) -Coagulation (fibrinogen, etc) -Immunological functions (globulins) - Inflammation Functions
-Total Proteins are low at birth 60-80% of adult values mainly due to lower globulins -Increase after colostral absorption serum protein concentration can assess colostral intake -Decline over next 1-5 weeks -Reach adult concentrations in 6-12 months Age Associated Changes N.B. Birds have lower reference intervals for total proteins (22-52 g/L) compared to mammals (54-75 g/L)
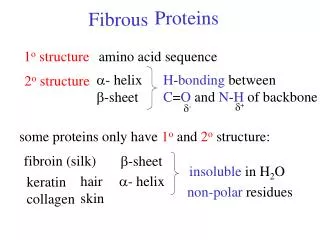
Globulins - and - Globulins: • Most are synthesised by the liver • Include: • Acute phase proteins of inflammation • Acute phase proteins (APP) are serum/plasma proteins whose concentrations change during inflammation. Most are increased (positive APP) and some are decreased (negative APP). Examples of APPs are fibrinogen, C-reactive protein (CRP) • Transport proteins (e.g. lipoproteins) • Some immunoglobulins (IgM, IgA) -Globulins: • Most immunoglobulins secreted by B lymphocytes and plasma cells in many tissues particularly the lymphoid organs
Protein Measurement -Refractometer Measures total proteins only Rapid, easy and reproducible results Best accuracy between 25-95g/L Falsely increased values in haemolysed & lipaemic samples -Spectrophotometric methods Biuret method (for Total proteins) Different dyes (for Albumin) • Refractometer measurement of total protein is less accurate than spectrophotometry but adequate for routine use. • In routine chemistry, globulin is not measured, only estimated (globulin = total protein–albumin)
Serum Protein Electrophoresis Interpretation is based on: 1.the morphology of the electrophoretical profile 2. the concentration of each fraction calculated from total proteins - + α1 α2 β1 β2 γ albumin globulins
Serum Protein Electrophoresis • Principle: Proteins migrate in an electrical field at a rate dependent on their net charge & molecular weight • Protein electrophoresis should not be performed in plasma because of fibrinogen interference. • Globulin fractions and subfractions can vary depending on the species and method used
Protein Abnormalities DYSPROTEINAEMIA: disturbance of the relative or absolute concentrations of proteins A. HYPERPROTEINAEMIA ( concentration of plasma proteins) B. HYPOPROTEINAEMIA ( concentration of plasma proteins)
Hyperproteinaemia 1. Hyperalbuminaemia - Dehydration is the only cause 2. Hyperglobulinaemia -Increased and globulins Acute Inflammation -Increased and globulins Chronic inflammation
Polyclonal gammopathy: Increase in multiple immunoglobulins Monoclonal gammopathy: Increase in a single immunoglobulin Increased Immunoglobulins Alb Alb
Hypoproteinaemia 1. Overhydration with intravenous fluids, polydipsia 2. Hypoalbuminaemia 3. Hypoglobulinaemia N.B. Overhydration with intravenous fluids or polydipsia will cause haemodilution (pseudohypoproteinaemia). Young animals (< 6-9 months) have lower reference values for proteins than adults
Hypoalbuminaemia: Causes • Inadequate protein intake Starvation Malabsorption/maldigestion Lactation • Decreased albumin synthesis: Hepatic insufficiency Acute Inflammation • Increased albumin loss: Renal Gastrointestinal Haemorrhage / Exudates
Hypoalbuminaemia • Inflammation can result in hypoalbuminaemia as albumin is a negative acute phase protein (i.e. albumin decreases in response to increased globulin and other acute phase proteins) • Renal disease = albumin losing nephropathy (amyloidosis or glomerulonephritis). Globulins not affected • Gastrointestinal = protein losing enteropathy (alimentary lymphoma, lymphangectasia, inflammatory bowel disease). Globulins also ↓ • Chronic haemorrhage. Globulins also ↓ • Exudates e.g. pyothorax, peritonitis. Globulins may ↑
Hypoglobulinaemia: Causes • Decreased globulin intake Colostrum deprivation Failure of passive transfer (neonates) • Decreased globulin synthesis Immunodeficiency diseases (↓ globulins) Hepatic insufficiency (↓ and globulins. Albumin also ↓) • Increased globulin loss Gastrointestinal Haemorrhagic
Fibrinogen • Consumed during blood clotting (not part of serum total protein assessment) • Produced by liver • Important in coagulation • Marker of inflammation
Hyperfibrinogenaemia caused by Inflammation Dehydration Hypofibrinogenaemia caused by Failure of production (Congenital or Severe hepatic insufficiency) Increased consumption (Disseminated Intravascular Coagulation) Overhydration Fibrinogen Abnormalities