Download
1 / 51
510 likes | 653 Views
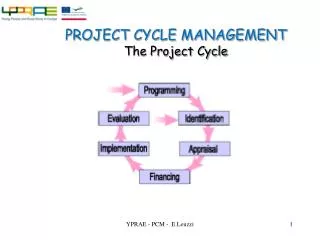
The Engagement Cycle. A new way of thinking about Patient and Public Engagement (PPE) in World Class Commissioning April 2009. 1. Introduction. Introduction. The Powerpoint pack contains the following sections:. 1. Introduction Purpose How the engagement cycle was developed

E N D
The Engagement Cycle A new way of thinking about Patient and Public Engagement (PPE) in World Class Commissioning April 2009
Introduction The Powerpoint pack contains the following sections: • 1. Introduction • Purpose • How the engagement cycle was developed • Policy context • Key principles of effective PPE • A conceptual framework for PPE • 2. The engagement cycle • Key PPE activities across the cycle • Customer insight • A conceptual framework for patient experience • Engagement culture and systems
Introduction How the engagement cycle was developed The engagement cycle has been developed by InHealth Associates, on behalf of the Department of Health. It is based on work carried out with Croydon PCT. It has been developed and tested with national stakeholders and the following organisations: NHS Coventry, Dudley PCT, NHS Sheffield, NHS Suffolk, West Sussex PCT. Thanks are also due to all stakeholders who fed back or contributed to thinking about the e-cycle. See final slide.
Purpose About the engagement cycle The engagement cycle is a way of approaching Patient and Public Engagement (PPE) in World Class Commissioning. It is a representational model that highlights who needs to do what to engage patients and the public at each stage of the commissioning cycle. It can be used to facilitate improvements in World Class Commissioning, particularly concerning Competency Three - engaging with patients and the public. The engagement cycle is not a toolkit, but a starting point for thinking about PPE in commissioning. It provides checklists for action and will be developed to include links to policy documents, case studies, toolkits and other materials. It has been used so far to undertake assessments of who is doing what at each stage of the cycle, to help develop action plans, identify learning and support needs and as a a basis for PPE strategies and organisational development plans.
Purpose About the engagement cycle • It can be used by different commissioners • Partner agencies undertaking PPE across the local health economy; • Primary Care Trusts developing corporate strategies and plans for commissioning and PPE; • Practice Based Commissioners; • Networks responsible for pathways of care for particular client groups; • Commissioning leads within PCTs responsible for particular client groups. • At a strategic level • Boards, Directors and senior managers can use and promote the engagement cycle as a planning tool. • At an operational level • Commissioning leads can work together with PPE leads to undertake the appropriate engagement activities at each stage of the cycle.
Policy context Policy context (1) Primary Care Trusts (PCTs) need to become ‘World Class Commissioners’, able to shift the NHS towards a more localised, personalised, responsive and accountable system. Competency Three of WCC states: “PCTs are responsible through the commissioning process for investing public funds on behalf of their patients & communities. In order to make commissioning decisions that reflect the needs, priorities & aspirations of the local population, PCTs will have to engage the public in a variety of ways, openly & honestly. They will need to be proactive in seeking out the views & experience of the public, patients, their carers & other stakeholders, especially those least able to advocate for themselves.” PPE is part of other competencies such as working with community partners (Competency Two) & leading the local NHS (Competency One). PCTs need to fully engage and involve patients & the public as citizens in a dialogue about health needs, strategic planning, service design & decision making & communicate with them to increase understanding & confidence in using local services.
Policy context Policy context (2) The NHS Constitution states: You have the rightto be involved, directly or through representatives, in the planning of healthcare services, the development and consideration of proposals for changes in the way those services are provided, and in decisions to be made affecting the operation of those services.. Section 242 of the consolidated NHS Act 2006 places a duty on NHS trusts, PCTs & strategic health authorities to make arrangements to involve patients and the public in service planning & operation, & in the development of proposals for changes. Real Involvement: working with people to improve healthcare provides guidance for PCTs and other NHS organisations to identify who they need to involve and what they need to do to deliver better involvement practices, to make sure the NHS is more locally accountable and shaped by the people who use it. World class commissioners will demonstrate their competence through having a coherent strategic plan underpinning their operational plan, Local Area Agreement (LAA), financial plan and workforce development strategy.
Key principles of effective PPE Key principles of high quality PPE • Be clear about what involvement means • Have a shared understanding of definitions and purpose • Ensure adequate resources - money, time and people • Focus on improvement • Demonstrate change as a result of engagement • Embed systems linking decision-making to impact • Ensure senior commitment and leadership • Support staff and equip them with the necessary skills • Be clear about why you are involving people • Clarify objectives & links to organisational priorities • Explain what can change & what is not negotiable • Use what is already known about people’s perspectives • Identify and understand your stakeholders • Define who needs to be involved & likely to be affected • Ensure activities are relevant to stakeholders’ interests • Involving people • Ensure that methods suit the purpose of engagement • Make special efforts to include seldom heard groups • Be clear how views will feed into decision-making • Provide feedback about action you intend to take • Ensure people have support to get involved
A conceptual framework for PPE Influence Feedback Information Individual My say in decisions about care and treatment Collective Our say in planning, design and delivery of services
OUTCOMES OUTCOMES OUTCOMES A conceptual framework for PPE
The engagement cycle The key PPE activities - Why & How…
The Engagement Cycle Engaging communities to identify health needs & aspirations Overview Commissioning organisations need to work with partners to engage communities in identifying their health needs and aspirations when developing strategic plans. This includes making sure community perspectives – people’s preferences, felt needs and expectations – are built into the Joint Strategic Needs Assessment (JSNA) and health needs assessments undertaken with particular communities. This means moving beyond a solely data-driven approach to needs assessment to one that is complemented by the views of those in the community.
The Engagement Cycle Engaging communities to identify health needs & aspirations Why – Rationale and benefits Policy and practice guidance emphasises joint working (e.g. Local Area Agreements) PCTs need to be local leaders of NHS S242 requires involvement in planning and development Contributes to long term area-wide vision and strategies Contributes to enhanced public health programmes Provides new ideas for meeting unmet needs Highlights what services are needed, where and how to better deliver them Promotes joint working – externally and internally Promotes accountability by showing the reasons why actions are being taken
The Engagement Cycle Engaging communities to identify health needs & aspirations How (1 of 2) Work together with all local partners (e.g. statutory partners, MPs, Health Scrutiny, Practice Based Commissioners, potential & current providers, Third Sector) Work with LINks Learn from needs assessment undertaken in specific areas Pool resources and bring together patient experience data trends, needs assessment and aspirations Focus attention on seldom heard groups where needs may be greatest and gaps in data common Work with intermediary organisations
The Engagement Cycle Engaging communities to identify health needs & aspirations How (2 of 2) Link with locality groups and neighbourhood management teams Build capacity for effective lay representation on Strategic Boards Adopt community development and participatory appraisal methods Understand customer insight techniques and drivers of behaviour. Utilise social marketing approaches Use public engagement exercises to reveal expectations and aspirations (e.g. Visioning, open-space, future search, whole-systems events, arts-based approaches)
The Engagement Cycle Engaging the public in decisions about priorities & strategies Overview Commissioning organisations need to engage with the public as citizens and taxpayers about the way resources are allocated in order to promote accountability and ensure services are planned fairly. This means having transparent processes by which decisions are made about prioritisation (e.g. what services are funded and what is not, how much is spent on which services), changes in services (i.e. that may require formal consultation) and long term commissioning strategies.
The Engagement Cycle Engaging the public in decisions about priorities & strategies Why – Rationale and benefits Statutory requirement for ongoing engagement Increased need for local accountability requires open and honest dialogue with local residents More robust decision making process can integrate different stakeholder perspectives Commissioning priorities and operational plans better reflect local aspirations Better decisions about what services are needed Contentious decisions based on informed and transparent dialogue Shared understanding of expectations, limitations, areas of consensus and tension Consistent two-way information flow between public and PCT with demonstrable impact of public feedback Improved reputation as local leader of the NHS through increased public confidence in local NHS decision making
The Engagement Cycle Engaging the public in decisions about priorities & strategies How (1 of 2) Ensure outcomes from needs assessment and community aspirations work feeds into strategic planning and decisions about priorities Use this stage of the cycle to promote and develop ongoing mechanisms for dialogue with local people Engage with stakeholders (including the media) openly about decision making process and reasons for decisions Work closely with Health Scrutiny and LINks Be clear about the similarities and differences between formal consultation and ongoing or informal engagement Develop criteria and framework for thinking about different types of prioritisation decisions (e.g. evidence-based decisions to fund or not to fund treatment; decisions about commissioning priorities; reconfiguration)
The Engagement Cycle Engaging the public in decisions about priorities & strategies How (2 of 2) Do not rely solely on lay representatives on advisory or partnership boards as sources of expertise or to rubberstamp decisions. Learn from good practice in local authorities and other partner agencies Make sure the views of seldom heard groups are incorporated into decision making Consider approaches that ensure a cross-section of local residents are involved Consider deliberative methods (i.e. that allow people to deliberate on complex information and that allow people to rank priorities)
The Engagement Cycle Engaging patients in service design & improvement Overview Commissioning organisations need to work with partners – including service providers, potential suppliers, clinicians and frontline staff – to engage patients, carers and families in co-designing (or redesigning) services. Much good work in this area is being undertaken. But more needs to be done to build on, and bring together, previous PPE work and patient experience data. It is crucial that outcomes from PPE work at this stage is carried forward into developing standards and outcome indicators within contractual agreements.
The Engagement Cycle Engaging patients in service design & improvement Why – Rationale and benefits Improvements in access to, and quality of, services, patient experience, satisfaction and outcomes Better co-ordinated care across health and social care Helps ensure quality is at heart of commissioning Reduced level of complaints and increased positive feedback leads to improved staff morale Service improvements and re-designs accepted and owned by public and patients S242 requires engagement in service planning & design PCTs need to better use patient experience data Patient Reported Outcome Measures (PROMs) will be increasingly important and are in 08/09 operating plans PCT needs to be local leaders – leading service improvement that fully engages patients, carers and families enhances reputation
The Engagement Cycle Engaging patients in service design & improvement How (1 of 2) Bring together existing patient experience data to help design services before embarking on new PPE work Ensure project initiation documents and business cases for improvement work include PPE and are resourced Align different initiatives (e.g. primary care redesign & client-specific pathway work). Use PPE as a trigger for breaking down silo working Work with local providers and potential suppliers – but be aware of conflicts of interest and procurement guidance Make sure clinical leaders, clinical and non-clinical staff are engaged in process Draw on good practice from service improvement initiatives
The Engagement Cycle Engaging patients in service design & improvement How (2 of 2) Learn from the many national and local examples of good PPE practice in pathway design Engage patients and carers in identifying solutions - not just about what’s going wrong or as subjects of research Engage patients in defining quality measures to be translated into contractual agreements and service standards Consider using a range of approaches - quantitative and qualitative (including stories, real time feedback, web 2.0) Think about how to capture and utilise the ‘1000s of everyday conversations’ at between staff, patients and carers Use one-off initiatives as trigger for sustained engagement
The Engagement Cycle Patient centred procurement & contracting Overview Commissioning organisations need to ensure that the learning from service design and pathway improvement work leads to outcomes that can be used to set standards and outcome measures. In turn this can be used within contracts and service level agreements. Patients and the public can be actively involved in developing tenders, helping to scan for innovation, identify potential providers, participating in tender processes and panels and making decisions on resources.
The Engagement Cycle Patient centred procurement & contracting Why – Rationale and benefits PCTs need to manage market and identify wider array of potential providers Service Level Agreements (SLAs) better reflect patient-centred indicators Focuses minds on identifying providers who can better meet needs of patients Performance metrics need to include more patient experience indicators Improved monitoring and performance monitoring flows from being able to specify outcomes that matter to patients Patient representation on tender evaluation panels leads to increased public confidence around providers
The Engagement Cycle Patient centred procurement & contracting How (1 of 2) Ensure evidence of what matters to patients derived from service redesign work is part of standards, outcome indicators and specifications within contracts Engage patients and the public in identifying providers who can deliver innovative solutions (e.g. voluntary sector, social entrepreneurs, social enterprises) Engage voluntary sector networks in identifying social innovation Engage and support patients and public in procurement processes – in developing tenders and as part of procurement panels
The Engagement Cycle Patient centred procurement & contracting How (2 of 2) Make sure there is clarity about patient representation on panels - their role, terms of reference and training Consider creative methods (e.g. Dragon’s Den) in procurement decisions Consider participatory budgeting approaches that allow enhanced public decision making over resources Involve people in the appointment of staff Hold briefing events so that the wider public find out what is going on and about proposals being developed
The Engagement Cycle Patient centred monitoring & performance management Overview PCTs need to work with local providers to gather and use patient-derived data concerning outcomes and experience in order to monitor and performance manage providers. This means ensuring that contracts and SLAs that specify outcomes and quality are followed up by systematic methods to gather and use patient experience data and patient-recorded outcome measures (PROMs). Patients themselves can also be supported to monitor services and undertake review visits.
The Engagement Cycle Patient centred monitoring & performance management Why – Rationale and benefits Identifies what’s working and what’s not in terms of quality of, and access to services Ongoing patient-centred monitoring promotes learning for improvement Increasing emphasis on commissioning for quality and outcomes Generates better quality data to augment needs assessment and aspirations work Patient Reported Outcome Measures (PROMs) are included in this year’s Operating Framework Leads to more efficient monitoring and performance management Provides increased opportunities to improve services (e.g. though incentivising quality)
The Engagement Cycle Patient centred monitoring & performance management How (1 of 2) Complement monitoring activity with regular meetings to discuss quality and outcomes Value and use patient-derived data (quantitative and qualitative) as much as routine data about activity Find ways to get timely patient experience data to those monitoring contracts Consider having patient representatives as part of regular monitoring meetings with providers Be clear about roles and responsibilities of commissioners and providers concerning who gathers, reports and uses patient experience data Adopt patient-centred methods for monitoring as well as patient-centred measures (e.g. Patient/user focused monitoring; Mystery shopping)
The Engagement Cycle Patient centred monitoring & performance management How (2 of 2) Work with LINks to ensure that data they have from visits to providers are incorporated into monitoring processes Develop ways to reward improvements in quality Consider real-time engagement via the use of hand-held patient experience equipment Utilise methods of online dialogue Find ways to empower clinical and non-clinical staff to gather and use data from everyday staff-patient contact Ensure that patient experience data gathered for monitoring processes are available to others (e.g. those planning needs assessments, priority setting, service redesign, etc).
The engagement cycle Customer insight
Customer insight Customer Insight Overview • Each of the key PPE activities should generate data about what matters to patients. This data can be ‘patient-derived’ (i.e. comes from patients directly or indirectly) or ‘patient experience data’ (i.e. is about people’s experiences of services). • Specialist customer insight techniques can also be used, such as segmentation, customer journey mapping, understanding the drivers of satisfaction and social marketing. • Commissioning organisations should have systems and processes in place to capture, use, bring together, report and learn from this data. This central insight function can then feed relevant data into other PPE activities around the engagement cycle. • Data should also be targeted to different audiences: • Boards (for strategic planning) • Performance Managers (for quality monitoring) • Improvement teams (for redesign work) and • Patients and the public (for accountability purposes)
Customer insight Customer Insight Why – Rationale and Benefits Vital Signs within Operating Framework require better capture and use of patient experience data Commissioners need to develop methods to incentivise quality improvement. Better use of patient experience data may save resources otherwise spent on duplicating PPE efforts Boards require an overview of what matters to patients and where improvements are needed to aid strategic planning, better governance and quality assurance Performance managers require timely data about quality for monitoring purposes Commissioning organisations need to be able to report back to patients and the public about what happened as a result of PPE – to adopt a ‘you said, we did’ communications culture
A framework for thinking about patient experience Customer Insight How – a conceptual framework for patient experience data • 1. Consider what matters to patients (the patient experience dimensions) • 2. Consider different sorts of data that can give insight into what matters to patients: • routine data • patient-derived data
A framework for thinking about patient experience What matters to patients • These things should be in place at all points during care and treatment… • Staying well (prevention, health promotion, self-care) • Getting better, feeling better (outcomes of care) • The right care from the right people (clinical quality, safety of treatment) • Treated as a human being (humanity of care) • Information, communication and having a say (involvement) • Being supported (incl. support for carers and relatives) • Safe, clean, comfortable place to be (environment of care)
A framework for thinking about patient experience What matters to patients • The following are about the ‘journey’ itself … • Right treatment at the right time (timely access) • Right treatment in the right place (physical access) • Not being passed from pillar to post (continuity of care) • Continuous care (after-care) • Support for independence (e.g. self-care)
A framework for thinking about patient experience What matters to patients • All these things matter to us, no matter who we are and regardless of circumstance… • Different people from different communities may have different sorts of barriers to getting what they need • Different sets of people may make different trade-offs between elements (i.e. access vs. quality) • Equalities and diversity issues are cross cutting themes … the following table provides a framework for thinking about patient experience data.
A framework for thinking about patient experience What matters to patients
The engagement cycle Engagement culture and systems
The Engagement Cycle Engagement culture & systems Overview Turning PPE into everyday practice relies on a culture and systems that value and embed PPE throughout the organisation. The engagement culture and systems is the hub of the engagement cycle and drives PPE activity at, and between, each PPE stage.
The Engagement Cycle Engagement culture & systems • Ensure there is senior commitment and leadership for PPE and a culture of engagement • Develop a strategy for engagement that is stitched into all areas of work • Have a consistent approach to engagement across the organisation – one that relies on thinking through the key principles of engagement • Make sure there are solid reporting & monitoring systems for PPE and outcomes from PPE as part of mainstream business • Allocate clear roles, responsibilities and accountabilities for engagement (e.g. identify director level, PPE lead, commissioner responsibilities) • Identify adequate resources, practical support and learning opportunities (e.g. for staff and lay representatives) • Make sure all PPE work is underpinned by principles of: • partnership working • qualities and diversity How – developing the foundations
Acknowledgements • InHealth Associates thanks everyone who helped during this project. • In particular: • Croydon PCT, NHS Coventry, Dudley PCT, NHS Sheffield, West Sussex PCT and NHS Suffolk • Richard Gleave, Graham Reid, Joan Saddler and Mary Simpson (DH) • Dave Barron and Jeanette Miller (NHS Sheffield) • Jessie Cunnett (PPI Solutions) • Sarah Dugan and Sam Hill (Dudley PCT) • Jo Ellins (HSMC, University of Birmingham) • Jennie Fisher (NHS Suffolk) • Angela Hamilton and Sarah Bronsdon (Yorkshire & Humberside SHA) • Julia Holding (West Midlands SHA) • Sam Hudson and Andrew Singfield (NHS Institute) • Jane Martin and Esther Peeple (NHS Coventry) • Emily Savin and Meerat Kaur (Westminster PCT) • Matt Rowe and Rachel Oxburgh (The Storm Digital) • Meredith Vivian (DH) who has contributed so much to the PPE Agenda over the years