Download
1 / 1
10 likes | 204 Views
(A). (B). COX10. PMP22 Ex3. PMP22 Ex2. 17p11.2 dosage and PMP22 sequencing analysis in a cohort of patients in the UK. James M Polke 1 , Matilde Laurá 2 , Sinéad M Murphy 2 , Mary G Sweeney 1 , Mary B Davis 1 , Mary M Reilly 2. Introduction. PMP22 Sequencing Results.

E N D
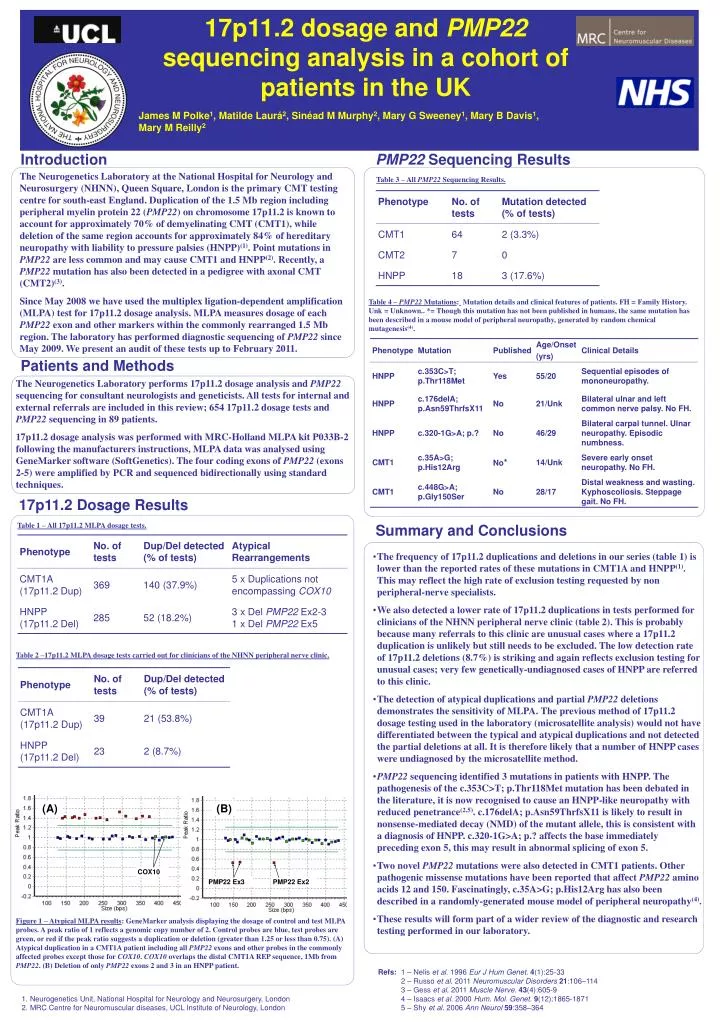
(A) (B) COX10 PMP22 Ex3 PMP22 Ex2 17p11.2 dosage and PMP22 sequencing analysis in a cohort of patients in the UK James M Polke1, Matilde Laurá2, Sinéad M Murphy2, Mary G Sweeney1, Mary B Davis1, Mary M Reilly2 Introduction PMP22 Sequencing Results The Neurogenetics Laboratory at the National Hospital for Neurology and Neurosurgery (NHNN), Queen Square, London is the primary CMT testing centre for south-east England. Duplication of the 1.5 Mb region including peripheral myelin protein 22 (PMP22) on chromosome 17p11.2 is known to account for approximately 70% of demyelinating CMT (CMT1), while deletion of the same region accounts for approximately 84% of hereditary neuropathy with liability to pressure palsies (HNPP)(1). Point mutations in PMP22 are less common and may cause CMT1 and HNPP(2). Recently, a PMP22 mutation has also been detected in a pedigree with axonal CMT (CMT2)(3). Since May 2008 we have used the multiplex ligation-dependent amplification (MLPA) test for 17p11.2 dosage analysis. MLPA measures dosage of each PMP22 exon and other markers within the commonly rearranged 1.5 Mb region. The laboratory has performed diagnostic sequencing of PMP22 since May 2009. We present an audit of these tests up to February 2011. Table 3 – All PMP22 Sequencing Results. Table 4 – PMP22 Mutations: Mutation details and clinical features of patients. FH = Family History. Unk = Unknown.. *= Though this mutation has not been published in humans, the same mutation has been described in a mouse model of peripheral neuropathy, generated by random chemical mutagenesis(4). Patients and Methods The Neurogenetics Laboratory performs 17p11.2 dosage analysis and PMP22 sequencing for consultant neurologists and geneticists. All tests for internal and external referrals are included in this review; 654 17p11.2 dosage tests and PMP22 sequencing in 89 patients. 17p11.2 dosage analysis was performed with MRC-Holland MLPA kit P033B-2 following the manufacturers instructions, MLPA data was analysed using GeneMarker software (SoftGenetics). The four coding exons of PMP22 (exons 2-5) were amplified by PCR and sequenced bidirectionally using standard techniques. 17p11.2 Dosage Results Table 1 – All 17p11.2 MLPA dosage tests. Summary and Conclusions • The frequency of 17p11.2 duplications and deletions in our series (table 1) is lower than the reported rates of these mutations in CMT1A and HNPP(1). This may reflect the high rate of exclusion testing requested by non peripheral-nerve specialists. • We also detected a lower rate of 17p11.2 duplications in tests performed for clinicians of the NHNN peripheral nerve clinic (table 2). This is probably because many referrals to this clinic are unusual cases where a 17p11.2 duplication is unlikely but still needs to be excluded. The low detection rate of 17p11.2 deletions (8.7%) is striking and again reflects exclusion testing for unusual cases; very few genetically-undiagnosed cases of HNPP are referred to this clinic. • The detection of atypical duplications and partial PMP22 deletions demonstrates the sensitivity of MLPA. The previous method of 17p11.2 dosage testing used in the laboratory (microsatellite analysis) would not have differentiated between the typical and atypical duplications and not detected the partial deletions at all. It is therefore likely that a number of HNPP cases were undiagnosed by the microsatellite method. • PMP22 sequencing identified 3 mutations in patients with HNPP. The pathogenesis of the c.353C>T; p.Thr118Met mutation has been debated in the literature, it is now recognised to cause an HNPP-like neuropathy with reduced penetrance(2,5). c.176delA; p.Asn59ThrfsX11 is likely to result in nonsense-mediated decay (NMD) of the mutant allele, this is consistent with a diagnosis of HNPP. c.320-1G>A; p.? affects the base immediately preceding exon 5, this may result in abnormal splicing of exon 5. • Two novel PMP22 mutations were also detected in CMT1 patients. Other pathogenic missense mutations have been reported that affect PMP22 amino acids 12 and 150. Fascinatingly, c.35A>G; p.His12Arg has also been described in a randomly-generated mouse model of peripheral neuropathy(4). • These results will form part of a wider review of the diagnostic and research testing performed in our laboratory. Table 2 –17p11.2 MLPA dosage tests carried out for clinicians of the NHNN peripheral nerve clinic. Figure 1 – Atypical MLPA results: GeneMarker analysis displaying the dosage of control and test MLPA probes. A peak ratio of 1 reflects a genomic copy number of 2. Control probes are blue, test probes are green, or red if the peak ratio suggests a duplication or deletion (greater than 1.25 or less than 0.75). (A) Atypical duplication in a CMT1A patient including all PMP22 exons and other probes in the commonly affected probes except those for COX10. COX10 overlaps the distal CMT1A REP sequence, 1Mb from PMP22. (B) Deletion of only PMP22 exons 2 and 3 in an HNPP patient. Refs: 1 – Nelis et al. 1996 Eur J Hum Genet. 4(1):25-33 2 – Russo et al. 2011 Neuromuscular Disorders 21:106–114 3 – Gess et al. 2011 Muscle Nerve. 43(4):605-9 4 – Isaacs et al. 2000 Hum. Mol. Genet.9(12):1865-1871 5 – Shy et al. 2006 Ann Neurol59:358–364 • Neurogenetics Unit, National Hospital for Neurology and Neurosurgery, London • MRC Centre for Neuromuscular diseases, UCL Institute of Neurology, London