Download
1 / 22
220 likes | 356 Views
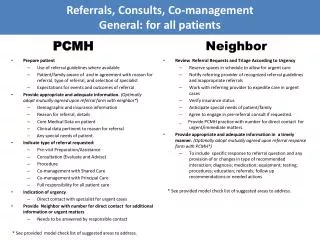
Session #E3a Friday, October 11, 2013. Community Partners and the PCMH. Roni Christopher, M.Ed., OTR/L, PCMH-CCE. Collaborative Family Healthcare Association 15 th Annual Conference October 10-12, 2013 Broomfield, Colorado U.S.A. Objectives for this Session. Define PCMH Tenets

E N D
Session #E3a Friday, October 11, 2013 Community Partners and the PCMH Roni Christopher, M.Ed., OTR/L, PCMH-CCE Collaborative Family Healthcare Association 15thAnnual Conference October 10-12, 2013 Broomfield, Colorado U.S.A.
Objectives for this Session • Define PCMH Tenets • Recognize opportunities for PCMH/Community Partnerships • Identify how such partnerships help to fulfill the pursuit of NCQA PCMH recognition • Identify the key components to a successful PCMH/Community Partner PCP extension program
THE TENETS OF THE PCMH • Person
The Opportunity and an Example • Pursuit of the NCQA PCMH certification is intense and can be challenging • The amount of responsibility on the PCP can feel overwhelming • We asked the question: • Can a successful model to build a community “extender” the PCP practice help the practice in the pursuit of PCMH? • Would such a relationship make a difference for our patients?
Creating the “Skunk Works” • We like skunks: “…a group within an organization given a high degree of autonomy and unhampered by bureaucracy, tasked with working on advanced or secret projects.”
Why Crossroads Makes a Good Skunk… • Crossroads make up • FQHC • In operation since 1992 • Inner-City Cincinnati
The Council on Aging as Another Skunk • Initial data exchanges with the COA • 6000 patient panel • 363 (6%) patients 60 years of age and older • 32 (8.8%) shared patients (Crossroad PCP patients receiving COA services) • Analyzed clinical outcome • Set shared goals
Current Model COA
160 patients over 60yrs 10,000+ patients 32 shared patients COA
Current Model COA
Shared Goals • Over-Arching Goals: • Formation of a relationship between COA and Crossroad, strengthened by close physical proximity and ease of communication. • COA to provide care coordination of Crossroad's senior patients in an effort to provide greater continuity of care. • CR to collaborate with COA to provide access to Primary Care services and ease of scheduling to patients COA is managing. • To develop a documentation system or process that reduces duplication of documentation for both COA and Crossroad. • Do ALL of the work to contribute to the NCQA PCMH recognition process
Look for Shared Goals • To show clinical outcome improvement in the following areas: • Hypertension (greater than 65% of hypertensive patients up to age 85 maintained below 140/90mmHg) • Diabetes (greater than 75% of diabetic patients with HgbA1C maintained at or below 9% - treatment goal is for A1C to be less than 8%) • Tobacco Use (greater than 95% of patients assessed for tobacco use and greater than 50% of smokers to receive smoking cessation counseling) • Behavioral Health (greater than 40% of patients up to age 65 to receive depression screen using the PHQ annually) • Lipid-Lowering Therapy (Greater than 86% of patients with diagnosis of CAD prescribed lipid-lowering therapy as indicated - treatment goal is for LDL to be less than 100) • Colorectal Screening (greater than 40% of patients 50 to 75 who have had a colonoscopy <=10y or sig<=5yrs or annual occult blood) • IVD (greater than 80% of patients with a dx of IVD on aspirin or other antithrombotic) • PAPs (greater than 75% of women 24 to 64 receiving one or more PAP tests at least every 2yrs) • Weight (greater than 60% of patients identified with BMI less than 20 or greater than 25 who have been counseled) • Decrease ED utilization and hospital admissions
CREATE THE HAND-OFF and HAND Back • Documentation and Collaboration Goals: • Self-management goals to be documented on all diabetic pts, hypertensive pts, and smokers • Treatment goals to be documented on all diabetic pts, hypertensive pts, and smokers • Assess barriers on patients and document • Follow-up on patients who have not had visits in a certain period of time • Conduct pre-visit preparation • Provide patient with written plan of care • Refer patients for additional care management • Reconcile medications at care transitions • Educate on new prescriptions • Track referrals • Counsel patients on healthy behaviors
Ask questions and look for partners • Model and Innovation Goals: • Identify the areas where time or resource prohibit primary care from doing “it all” • Look for partners who could do “it” and do “it” well • Identify current pattern with those partners • Look for a “win-win” pattern with those partners • Test what will/won’t work • Put it in play • DO NOT ASSUME THAT ANYONE BUT YOURSELF UNDERSTANDS WHAT A PCMH REALLY IS! • (maybe not even yourself?)
Why was the COA Interested? • Taking a leading role in healthcare transitions for adults • Wanting to understand how to maximize their products • Had services to offer, but did not understand what was needed at the PCP level
Where They are Now… • Initial stages • Hired RN Care Coordinator • Prepared office space • Monitoring key clinical metrics • Handing off and handing back… • Improving coordination for existing shared patients
Where We are Now… • Future Stages • Recruit Crossroad patients into COA programs • Recruit COA patients without a medical home into Crossroad • Measure outcomes for improvement
Lessons Learned • Being a PCMH = learning how to care for the patients who aren’t in your waiting room • Trying to do it “all” is an exercise in futility • There are community partners who truly want to partner • Don’t assume that their desire to partner equates to knowledge about what you need
Q&A and Contact Roni Christopher, M.Ed, OTR/L, PCMH-CCE • ronichristopher@yahoo.com