Download
1 / 40
400 likes | 506 Views
Identifying likely syphilis transmitters: Implications for control & evaluation*. Stuart M Berman, MD, ScM Division of STD Prevention CDC, Atlanta, GA. *Awaiting publication in Sexually Transmitted Diseases.

E N D
Identifying likely syphilis transmitters:Implications for control & evaluation* Stuart M Berman, MD, ScM Division of STD Prevention CDC, Atlanta, GA *Awaiting publication in Sexually Transmitted Diseases. Authors: Richard H. Kahn, Thomas A Peterman, Janet Arno, Emmet John Coursey, and Stuart M Berman
Background Major syphilis case detection strategies in the United States: Partner notification STD clinic Dx/Rx Private provider testing/diagnosis Broad screening (premarital, military, prenatal) Targeted screening (jails, bathhouses) Implicit assumption: every ‘early’ case found/Rx’d contributes equally to control But prevention potential varies among cases Little evaluation of detection strategies and their prevention potential
Goals • Determine which approaches were best for finding those syphilis cases that would contribute the most to disease control. • i.e, finding cases of high prevention value • “High prevention value”: • treatment was provided early in course of disease • individual was likely to expose multiple partners
Methods • Retrospective evaluation of data from 2 cities with heterosexual syphilis epidemics • Nashville and Louisville were cities with dramatic increases that had come under control
Sites: Response to epidemic Indianapolis, IN jail screening improve partner notification (including cluster interviewing) enhanced community partnerships emergency department screening Nashville, TN jail screening improve partner notification enhanced community partnerships
Methods: Source Data Routinely collected data (local level) - Interview records - Laboratory records - Morbidity reports
Methods: Coding Case Detection Detection Method??
Methods: “High prevention value” • Prevention value “score” for each case = Relative magnitude of transmission if case had not been identified: Relative # infectious days prevented by Rx X Expected number of (future) partners
Methods: “High prevention value” • Prevention value “score” for each case = Relative magnitude of transmission if case had not been identified: Relative # infectious days prevented by Rx X Expected number of (future) partners
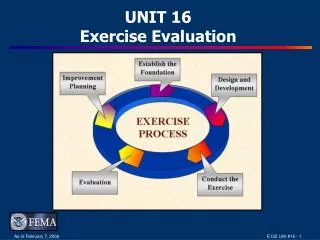
365 days exposure primary secondary latent latent 184 days 25 12 34 110 .24 probability of recurrence to secondary
365 days exposure primary secondary latent latent 184 days 25 12 34 110 .24 probability of recurrence to secondary • Assume diagnosis occurs in the middle of a stage; • Infectiousness occurs only during primary and secondary • Then the number of infectious days prevented by stage are:
365 days exposure primary secondary latent latent 184 days 25 12 34 110 .24 probability of recurrence to secondary Assuming diagnosis occurs in the middle of a stage, and infectiousness occurs only during primary and secondary, the number of infectious days prevented by stage are: Stage of DiagnosisPrimarySecondary RecurrenceTotal infectious days prevented Primary 6 110 26 (.24 x 110) 142 Latent before secondary 110 26 (.24 x 110) 136 Secondary 55 26 (.24 x 110) 81 Latent after secondary 13 (.12 x 110) 13 Relative number of infectious days prevented: Primary 142 days = 4.3 Secondary 81 days = 2.5 *Latent 33 days = 1 *Total duration of latent is 34+184=218 days. 34/218=.16 of latent is before secondary and 184/218=.84 is after secondary. Thus, the weighted average for latent is .16x136 days +.84x13 days = 33 days.
365 days exposure primary secondary latent latent 184 days 25 12 34 110 .24 probability of recurrence to secondary Assuming diagnosis occurs in the middle of a stage, and infectiousness occurs only during primary and secondary, the number of infectious days prevented by stage are: Stage of DiagnosisPrimarySecondary RecurrenceTotal infectious days prevented Primary 6 110 26 (.24 x 110) 142 Latent before secondary 110 26 (.24 x 110) 136 Secondary 55 26 (.24 x 110) 81 Latent after secondary 13 (.12 x 110) 13 Relative number of infectious days prevented: Primary 142 days = 4.3 Secondary 81 days = 2.5 *Latent 33 days = 1 *Total duration of latent is 34+184=218 days. 34/218=.16 of latent is before secondary and 184/218=.84 is after secondary. Thus, the weighted average for latent is .16x136 days +.84x13 days = 33 days.
365 days exposure primary secondary latent latent 184 days 25 12 34 110 .24 probability of recurrence to secondary Assuming diagnosis occurs in the middle of a stage, and infectiousness occurs only during primary and secondary, the number of infectious days prevented by stage are: Stage of DiagnosisPrimarySecondary RecurrenceTotal infectious days prevented Primary 6 110 26 (.24 x 110) 142 Latent before secondary 110 26 (.24 x 110) 136 Secondary 55 26 (.24 x 110) 81 Latent after secondary 13 (.12 x 110) 13 Relative number of infectious days prevented: Primary 142 days = 4.3 Secondary 81 days = 2.5 *Latent 33 days = 1 *Total duration of latent is 34+184=218 days. 34/218=.16 of latent is before secondary and 184/218=.84 is after secondary. Thus, the weighted average for latent is .16x136 days +.84x13 days = 33 days.
365 days exposure primary secondary latent latent 184 days 25 12 34 110 .24 probability of recurrence to secondary Assuming diagnosis occurs in the middle of a stage, and infectiousness occurs only during primary and secondary, the number of infectious days prevented by stage are: Stage of DiagnosisPrimarySecondary RecurrenceTotal infectious days prevented Primary 6 110 26 (.24 x 110) 142 Latent before secondary 110 26 (.24 x 110) 136 Secondary 55 26 (.24 x 110) 81 Latent after secondary 13 (.12 x 110) 13 Relative number of infectious days prevented: Primary 142 days = 4.3 Secondary 81 days = 2.5 *Latent 33 days = 1 *Total duration of latent is 34+184=218 days. 34/218=.16 of latent is before secondary and 184/218=.84 is after secondary. Thus, the weighted average for latent is .16x136 days +.84x13 days = 33 days.
365 days exposure primary secondary latent latent 184 days 25 12 34 110 .24 probability of recurrence to secondary Assuming diagnosis occurs in the middle of a stage, and infectiousness occurs only during primary and secondary, the number of infectious days prevented by stage are: Stage of Diagnosis Primary Secondary Recurrence Total infectious days prevented Primary 6 110 26 (.24 x 110) 142 Latent before secondary 110 26 (.24 x 110) 136 Secondary 55 26 (.24 x 110) 81 Latent after secondary 13 (.12 x 110) 13 Relative number of infectious days prevented: Primary 142 days = 4.3 Secondary 81 days = 2.5 *Latent 33 days = 1 *Total duration of latent is 34+184=218 days. 34/218=.16 of latent is before secondary and 184/218=.84 is after secondary. Thus, the weighted average for latent is .16x136 days +.84x13 days = 33 days.
Methods: “High prevention value” • Prevention value “score” for each identified case = Relative magnitude of transmission if case had not been identified: Relative # infectious days prevented by Rx X Expected number of (future) partners
Methods: “High prevention value” For expected number of future partners: Used number of critical period sex partners Primary = 4.3 x number of interview period partners (3m) Secondary= 2.5 x number of interview period partners (6m) Early latent= 1 x number of interview period partners (12m) o Number of interview partners was similar regardless of stage used
Methods: “High prevention value” Primary = 4.3 x number of interview period partners (3m) Secondary= 2.5 x number of interview period partners (6m) Early latent= 1 x number of interview period partners (12m) High prevention value: >10 Stage Sex partners Primary ≥ 3 (3 months) Secondary ≥ 5 (6 months) Early latent ≥ 11 (12 months)
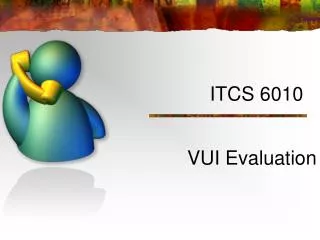
Finding high value cases:Women with early syphilis, Indianapolis
Finding high value cases:Women with early syphilis,Indianapolis
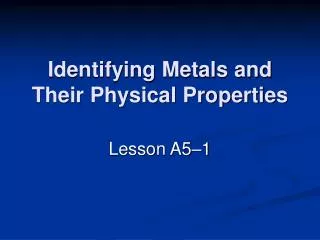
Finding high value cases:Men with early syphilis,Indianapolis
Finding high value cases:Men with early syphilis,Indianapolis
Finding high value cases:Women with early syphilis, Nashville
Finding high value cases:Women with early syphilis, Nashville
Limitations • Parameter estimates are from old studies; still valid? • Depends upon estimation of future number of partners; valid? • Assumes consistent classification of cases across sites; Jails?
Conclusions • For women: jail screening best for high-value cases (both sites) • For men: STD clinic was the important site for high-value cases (both sites) • Partner notification/cluster: Relatively few high value cases (Note: Didn’t assess contribution of preventive treatment provided to exposed but seronegative partners)
Conclusions (con’t) • Primary cases: relatively large contribution (esp for males) • EL cases: contributed few high-value cases among males; greater contribution among females (greater number of partners) • Approach may help to focus efforts on finding high value cases • Plan to evaluate approach in other contexts: MSM outbreaks, uncontrolled outbreaks, etc
The findings and conclusions in this presentation are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention/the Agency for Toxic Substances and Disease Registry