Download
1 / 75
760 likes | 1.03k Views
LOWER UROGENITAL TRAUMA. Yehya Elshebiny Adan Hospital . Bladder. Urethra. Genital. Bladder Injuries. External trauma ( 82%) RTA Falls, industrial trauma , blows to lower abdomen . Penetrating injury 60-90 % have associated pelvic fracture .

E N D
LOWER UROGENITAL TRAUMA YehyaElshebiny Adan Hospital
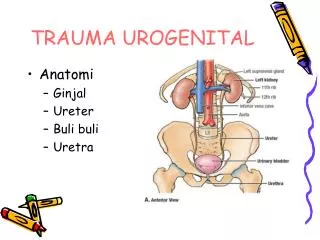
Bladder. • Urethra. • Genital.
Bladder Injuries • External trauma (82%) • RTA • Falls, industrial trauma , blows to lower abdomen . • Penetrating injury • 60-90 % have associated pelvic fracture . • 44% have associated intra-abdominal injury . • Only 3.5% of pelvic fracture have associated bladder Injuries . Types : Extraperitoneal (50-70% ) . almost always with fracture pelvis . ? Sharp bone edges . Intraperitoneal ( 25-40%). Combined (10-15%).
Iatrogenic trauma (17%) • External : Obstetric and gynaecologic procedures. General surgical and urologic interventions. • Internal : TURB.
Risk factors : • Intra-peritoneal : driving under the influence of alcohol • Extra peritoneal : disruptions of the pelvic circle • Iatrogenic : Previous CS . Previous pelvic surgery . Malignancy . Endometriosis . Sling procedures retropubicroute .
Presentation : • External trauma : bladder injury might be blurred by associated pelvic fracture and visceral injuries . • The cardinal sign of bladder injury is gross haematuria . • the classic combination of pelvic fracture and gross haematuria constitutes an absolute indication for further imaging of the bladder • Isolated gross haematuria or pelvic fracture, decision for further imaging should be based on the presence of other clinical signs and symptoms .
Other signs and symptoms : • Abdominal tenderness . • Abdominal distension . • Inability to void . • Extravasation of urine : extraperitoneal . uraemia .
Iatrogenic trauma . • During open surgery : methylene blue . • During TURB . • Postoperative : urine leakage from the wound.
Imaging : Cystography (conventional or CT) . Look for signs of associated urethral injury before catheter insertion .
Cystoscopy Routine postoperative cystoscopy after gynaecological procedures remains controversial. It is recommended for all procedures where bladder injury is suspected . ex. suburethral sling operations by retropubic route .
Ultrasound alone is insufficient . • Excretory phase of CT or IVP ??? Insufficient .
Treatment External injury : Blunt trauma: extraperitoneal rupture catheter drainage alone However : Open surgery #Orthopaedic surgery . # Surgical exploration for other injuries . # Bladder neck involvement, the presence of bone fragments in the bladder wall, concomitant rectal injury .
Blunt trauma: intraperitoneal rupture surgical repair laparoscopic suturing Penetrating injuries : emergency exploration
Iatrogenic injuries : Perforations recognisedintraoperatively are primarely closed IF not recognised : Extraperitoneal injuries : Bladder drainage and antibiotic prophylaxis. Intraperitoneal injuries surgical exploration with repair . In selected cases : continuous bladder drainage , antibiotic, and intraperitoneal drain . If after TURB : Immediate intravesical instillation with chemotherapeutic agents should not be performed . Meticulous bowel inspection is required to rule out concomitant injury .
Postoperative management Bladder catheter is maintained for 7-14 days. Cystography upon removal of the catheter is advised .
In Conclusion : • Extraperitoneal bladder perforations are more frequent than intraperitoneal perforations, mostly associated with pelvic fractures due to an RTA . • The combination of pelvic fracture and gross haematuria is highly suggestive of bladder injury , is a strong indication for Cystography . • Requires drainage with antibiotics . • Intraperitoneal bladder injuries require exploration and repair.
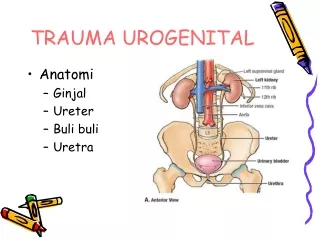
URETHRAL TRAUMA Anterior urethral injuries : Blunt trauma • Accounts for more than 90% • ‘Fall-astride’ or ‘straddle’ injury • Penile fracture : 20% have associated urethral injury . • Constriction device : ischaemic injuries . Penetrating injuries Iatrogenic urethral injuries caused by instruments are by far the most common cause of urethral trauma
Posterior urethral injuries : • Occurs in 4-19% of pelvic-fracture in males . • Found 0-6% in females ; Short and mobile, without any significant attachments to the pubic bone.
Diagnosis : Bleeding per urethra and voiding difficulty …. suspicion of urethral trauma, although their absence does not rule out urethral injury. Other signs : Haematuria Pain on urination - Dysuria Inability to void Haematoma Swelling ‘High-riding’ or “absent” prostate Blood at the vaginal introitus .
Retrograde urethrography Is the gold standard for evaluating urethral injury. • Ultrasonograph : Suprapubic catheter insertion . Tunica albuginea ruptures . • CT , MRI , and urethroscopy : have no place in the initial assessment of urethral injuries However, in females , urethroscopy helps in identification and staging of urethral injuries .
Management : The management of urethral injuries remains controversial because of the variety of injury patterns, associated injuries and treatment options available.
Anterior urethral injuries Blunt :suprapubic diversion Acute or early urethroplasty is not Indicated. Delayed management at 3-6 months : # Optical urethrotomy or urethral dilatation . # Anastomoticurethroplasty . # Flap/graft urethroplasty.
Fracture penis with urethral injury open repair .
Penetrating anterior urethral injuries : • Immediate exploration and end-to-end anastomosis Urethral debridement should be kept to a minimum since the spongiosum is well vascularised and so usually heals well. Peri-operative antimicrobial cover. • There is no role for acute placement of a graft or flap in the initial management of any urethral injury • Delayed management : If defect is > 1-1.5 cm in length, two-stage urethral repair.
Posterior urethral injuries Blunt injury : Partial tear • Acute management suprapubic or urethral catheter • Delayed Management # Urethral dilatation # Optical urethrotomy # Anastomoticurethroplasty
In complete urethral ruptures : The gap betweenthe disrupted end of the urethra retract and fibrous tissue fills the space between them. There is no urethral wall in the scarred space, and any lumen represents merely a fistulous tract between the urethral stumps .
Injury to the posterior urethra is most likely to occur with unstable pelvic fractures : • Bilateral ischiopubicrami fractures (‘straddle fracture’), • Symphysis pubis diastasis. • The combination of straddle fractures with diastasis of the sacroiliac joint has the highest risk of urethral injury .
Never life-threatening . • Strictures, Incontinence and Erectile dysfunction. • Erectile dysfunction occurs in 20-60% of cases . • Bilateral pubic rami fractures are the most frequent cause of impotence. • Neurogenic, due to bilateral damage of the cavernous nerves at the prostatomembranous urethra behind the symphysis pubis .
Management Complete posterior urethral rupture : suprapubic catheter is the primary treatment. Further treatment depends on the patients comorbidity and co-existing injuries .
When urethral trauma is suspected ,urethrogram is done then an attempt of urethral catheterisation should be carried. It is extremely unlikely that gentle passage of a urethral catheter will do any additional damage . Although it has been suggested that passing a catheter may convert a partial tear Into a complete one , there are no convincing data indicating that there is a higher rate of infection or urethral stricture after a single attempt at catheterisation . In an unstable patient, an attempt to pass a urethral catheter should be performed, but if there is any difficulty, a suprapubic catheter should be placed using US guidance .
Acute treatment options : after position of the suprapubic catheter include: