Download
1 / 65
660 likes | 787 Views
Dental Early Intervention in North Carolina. Rebecca King, DDS, MPH Chief, Oral Health Section NC Division of Public Health, DHHS 919-707-5487 Rebecca.King@ncmail.net. Turn of the Century. 1910 -- Dr. RM Squires: function ... prevent rather than cure

E N D
Dental Early Intervention in North Carolina Rebecca King, DDS, MPH Chief, Oral Health Section NC Division of Public Health, DHHS 919-707-5487 Rebecca.King@ncmail.net
Turn of the Century • 1910 --Dr. RM Squires: function ... prevent rather than cure • 1918 – NC Dental Society gets legislative funding • Reduce pain and infection • Educate on importance of oral health
Oral Health Section Staff • 6 Public health dentists • 58 Public health dental hygienists • 3 Health educators • 3 Equipment technicians • Support staff
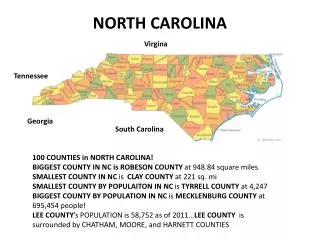
Oral Health Section Regions and Staff Assignments Central 10 Hygienists 4 Local Hygienists 22 Counties CAM- DEN ALLE- GHANY CURRITUCK GATES NORTH- AMPTON ASHE WARREN SURRY HERT- FORD STOKES ROCKING- HAM CASWELL VANCE PER- QUIMANS PERSON PASQUO- TANK GRAN- VILLE HALIFAX WATAUGA WILKES CHO- WAN ORANGE BERTIE MITCHELL YADKIN FORSYTH FRANKLIN AVERY GUILFORD YAN- CEY CALDWELL NASH ALEX- ANDER ALA- MANCE DURHAM EDGE- COMBE DAVIE WASH- INGTON MADISON IREDELL DAVID- SON DARE MARTIN TYRRELL WAKE BURKE WILSON BUN- COMBE CHATHAM RANDOLPH HAY- WOOD CATAWBA MCDOWELL BEAU- FORT PITT ROWAN SWAIN HYDE JOHNSTON LINCOLN RUTHER- FORD GREENE LEE GRAHAM HENDER- SON CABARRUS JACK- SON WAYNE HARNETT CLEVE- LAND MONT- GOMERY TRAN- SYLVANIA GASTON LENOIR MOORE STANLY POLK MACON CHEROKEE CRAVEN MECKLEN- BURG PAM- LICO CLAY JONES SAMPSON CUMBER- LAND RICH- MOND HOKE DUPLIN UNION ANSON SCOT- LAND CARTERET ONSLOW Western 21 Hygienists 1 Field Dentist 2 Local Hygienists 40 Counties ROBESON BLADEN PENDER NEW HANOVER COLUMBUS BRUNSWICK Eastern 19 Hygienists 1 Field Dentist 1 Local Hygienist 38 Counties Hygienists Field Dentists Supervisors Local Hygienists Under State Supervision Revised 9/05
Program Components • Dental disease prevention • Oral health assessment • Dental health education and promotion • Access to dental care • Dental public health residency
1 Dental Disease Prevention • Water fluoridation • Preschool dental preventive programs • Dental sealants • Fluoride mouthrinse
Water Fluoridation NC: 85% on municipal water supplies receive the benefits of water fluoridation
Preschool Dental Preventive Programs Much more later.
Dental Sealants • Statewide goal is 50% - a top OHS priority • OHS target population • K-3 high-risk children • 15,000 per year • Fifth graders with sealants increased from 28% (1996) to 44% (2006)
Fluoride Mouthrinse • School-based program from mid-1970s to 2002 • Increasingly targeted in early 1990s • Discontinued due to budget cuts and lack of recent data
Fluoride Mouthrinse Resurgence • Survey data showed decreased disparities • Obtained expansion budget funding in 2006 • Targeting schools with highest decay rates who promise compliance • Plan to begin rinsing in January 2007
2 Oral HealthAssessment • Statewide dental surveys • Oral health surveillance
Statewide Dental Surveys Provide evidence base for program: • Early 1960s • 1976-1977 • 1986-1987 • 2003-2004
2003-2004 Statewide Dental Survey • Sample: 8000 children K-12 • Study how well NC decay prevention programs are reducing decay • Measure • Disparities • Parents’ knowledge and opinions • How dental health affects quality of life • Results used for Section strategic planning
Select Survey Findings • Rates of decay in preschoolers have deteriorated slightly. • Past improvements in decay rates in permanent teeth have leveled off. • Whites (19%) are least likely to have untreated decay, followed by blacks (30%), then “Others” (mostly Latinos) (38%). • Not including early decay (non-cavitated lesions) underestimates disease levels by 35-40%. • 40% do not think baby teeth are important.
Trends in Untreated Decay in Permanent Teeth Percent Year NC OHS Statewide Dental Survey Data
Oral Health Surveillance Calibrated dental assessments • By PH RDHs • Grades K and 5 • County oral health status data • Referral for treatment needs
Surveillance Results • 21% K, 5% fifth graders have untreated decay • Proportion of kindergartners who have had tooth decay has increasing, maybe leveling off • Proportion of fifth graders who have had tooth decay is low but fluctuating • Fifth graders with sealants increased from 28% to 44% (1996-97 to 2005-06)
3 DentalHealth Education • School-based education and • Community outreach • Professional education • Educational materials
School-based Education • 176,000 children thru classroom education • 16,600 Adults • Parent education • Teacher support • Also health professionals
Exhibit Promotions Aging, consumerism, diabetes, careers, sealants, early childhood caries, fluorides, oral hygiene, nutrition, tobacco, injury prevention, OHS program
4 Access to Dental Care • Referral/follow-up for care • Improved access for low-income families • “Under direction” activities
Oral Health Surveillance • Referral for treatment needs • >129,000 K,5 screened • Identified >28,400 in need of dental care • Helped get dental care for 10,800 • Additional 67,800 screened for sealants, GKAS! and at request of school nurses
Improved Access • 1999 NC IOM Task Force on Dental Care Access had 23 recommendations, e.g. • Increased fees for Dental Medicaid services • Funding for physician-based dental preventive services • “Under Direction” • Medicaid Dental Advisory Committee (PAG) • Licensure by credentials • 2005 NC Oral Health Summit – latest update and new action steps
2006 Give Kids a Smile! • NC Dental Society initiative to provide free dental care for underprivileged children • To date: • 7000 volunteers • 54,000 children served • > $4 million free care • OHS PH Dental Hygienists screen and coordinate
Local Dental Safety Net Clinics • OHS provides TA for new clinics • OHS provides temporary dentist coverage on limited basis • Number increased dramatically from the early 1990s to 114 fixed, mobile and “free” clinics in 2005
5 Dental Public Health Residency • Training for dental public • health specialists • Growth for the Division
Smart Smiles An Appalachian RegionalCollaborative Partnership to Improve Dental Health
The Beginning • Appalachian Regional Consortium/NC Partnership for Children/Smart Start health assessment (fall 1996) • 1/3 kindergarten children in western part of state had untreated decay • Primary need • reduce early childhood caries • improve dental health
Motivating Assumptions • ECC is a serious public health problem • Its burden can be reduced through prevention targeted to very young, high risk children • Virtually all infants & toddlers obtain care at medical offices and it is a logical place to provide services
Additional Assumptions • Physicians and their staff know that ECC is a problem and they are willing to help prevent it • Primary medical care providers need help to learn procedures and to implement them in their practices • Innovations must be evaluated for adoption rates, quality of care, clinical effectiveness, costs and political concerns
Fluoride Varnish Safety and Effectiveness • Safe, easy to use and accepted • No studies of effectiveness in 1-2-year-olds • Emerging evidence of effectiveness in primary teeth of older children • Supported by a larger body of evidence • effective in permanent teeth • other topical fluoride applications are effective
Local community leaders State and regional Smart Start agencies NC Oral Health Section UNC School of Dentistry UNC School of Public Health Ruth & Billy Graham Health Center Local health departments Pediatric offices Partners/Advisory Board
Medical Community Preparation • Worked with licensing boards: • medical • dental • nursing • Sample standing orders
Smart Smiles Preventive Package • Medical setting • targeted oral health education for caregivers • dental screening • fluoride varnish application • First visit ~ age 9 months • Repeat every 6 months until age 3
Why Preventive Medical Model? • This is where young children are • Multiple services at one visit • Most general dentists uncomfortable seeing children this age • Interest and willingness of medical community • Few pediatric dentists • Treatment is expensive • This was the best idea anyone had
Targets • Children, 9 - 36 months, high risk for caries. • Medical risk factors & socioeconomic indicators • families 200% Federal Poverty Level • medically compromised children • older siblings with poor oral health
Challenges • Effectiveness • identifying the high risk children • getting them in for the service on a regular schedule • Financing • grant stipulated that providers provide service at no cost to patients • economics was an issue for medical practices
Effectiveness Issues • Provide services to high risk children • 80-85% decay in 20-25% children • Begin prevention before decay begins (~ 9 months) • Provide services on a regular basis
Finances Medicaid agreed to reimburse (July 1999) • Medical offices - required training, recognized Smart Smiles trainers • Six visits between 9 months and age 3 (90 day interval) • Reimburse for: • dental health education for parent/care-give • oral screening and referral for child • fluoride varnish application for child
Smart Smiles Evaluation (8/2001) • $2.2 million, 5 year grant • NIDCR, National Institutes for Health • Effectiveness - does program reduce cavities? • Does it work in this setting? • Can we provide package frequently enough? • Data collection completed
Smart Smiles Evaluation Aims • Short term effects on cavities (dmf scores) in 3-year-old children • Intermediate effects on cavity-related treatments, Medicaid costs, hospital use, and quality of life • Longer-term effects on cavities in 5-year-old children after 2-year gap in services
Into The Mouths of Babes Statewide Medicaid Dental Prevention Program for Young Children
Goals • Increase access to preventive dental care for low-income children • Reduce the prevalence of ECC in low-income children • Reduce the burden of treatment needs on a dental care system already stretched beyond its capacity to serve young children
IMB Statewide Pilot • December 1999 • Pediatricians and family practitioners • Used Smart Smiles training session and educational materials, modified over time • Added training on billing procedures
Statewide IMB Progression • Pilot – volunteer trainers • June 2000, RFA from HCFA to Medicaid agencies for Innovative ECC program • partners: Medicaid, UNC Schools of Public Health and Dentistry, NC Pediatric Society, NC Academy of Family Physicians, Oral Health Section • evaluate level of training required for MDs
Dental Support • Fall 1999 NC Academy of Pediatric Dentistry endorsement • Spring 2000 NC Dental Society resolution of support • Fall 2001 NC Academy of Pediatric Dentistry reaffirmed support