Download
1 / 26
260 likes | 395 Views
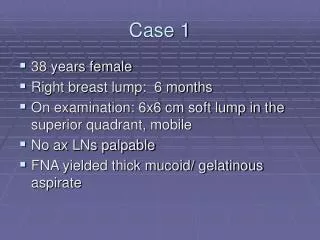
UBC-Case 1. Samuel Yip PhD, MD, FRCPC Western Stroke Day 2012. History. 30 year old RH female Recently from UK While pushing herself off a table, sudden onset of left hemiplegia and decrease LOC 6 months ago she had1 spell of sudden onset of dizziness

E N D
UBC-Case 1 Samuel Yip PhD, MD, FRCPC Western Stroke Day 2012
History • 30 year old RH female • Recently from UK • While pushing herself off a table, sudden onset of left hemiplegia and decrease LOC • 6 months ago she had1 spell of sudden onset of dizziness • No neck pain and no neck trauma • No SOB and no leg pain
History • No other stroke risk factors • Non-smoker • No Family history of stroke • OCP (12 yrs) for Endometriosis
Examination • Initial Examination: • AVSS • Mild decrease in left nasolabialfold • Left deltoid weakness of 4+; no drift • NIHSS = 1
Too Good to Treat NHD = No Home Discharge
TREATMENT OPTIONS • Iv-tPA • Heparin • ASA +/- Plavix • ASA +/- Plavix + Heparin • Enroll into a RCT – TEMPO-1
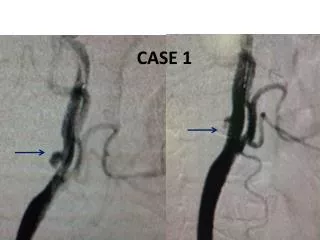
BASELINE CTA Fluids, ASA, Heparin sc 24 hr CTA
Case Cont: Investigations • TTE and TEE showed • Large PFO • Spontaneous Right to Left shunt • Hypercoagulable workup was negative • Pelvic and Leg U/S showed no DVTs
Diagnosis • ? Paradoxical Embolism • Hepatic Hemangioma – Large venous lakes with potential stasis • 2 case reports suggesting hemangioma causing pulmonary embolism • Recent travel • Valsalvamaneuver • Large spontaneous right left shunt
Secondary Prevention • Stop OCP • ASA 81 mg once a day • Coumadin • Coumadin then PFO Closure
PFO and Stroke: Atrial septum – overlapping of the septum primum and septum secundum. When the fusion of these 2 structures fails, then a patent foramen is formed. This act as conduit for R to L shunt in adult life.
PFO and Cryptogenic Stroke • 25% of general population have a PFO • ~ 40% of young cryptogenic stroke patients have a PFO Overall et al., 2000
PFO and Stroke:Pathophysiology • Paradoxical Embolism
Paradoxical Embolism LA IAS T AO RA Srivastavaetl., NEJM 1997
PFO and Stroke:Pathophysiology • Paradoxical Embolism • Atrial Vulnerability – Paroxysmal Atrial Fibrillation • Endothelial dysfunction
PFO and cryptogenic stroke:Natural History • Risk of recurrent stroke is low • ~ 0.5 to 1% per year. (From recent cohort study and placebo randomized control trials ).
PFO in Cryptogenic Stroke Study (PICSS) • Substudy of WARSS (Multicenter, randomized, DB study, ASA (325 mg) vs Warfarin (mean INR 2.1); n = 2206) • Excluded symptomatic carotid and cardioembolic stroke • 630 patients underwent TEE • 42% had a cryptogenic stroke • 39% of the cryptogenic stroke had a PFO • Primary end point: recurrent ischemic stroke or death in 2 years Homma et al., Circulation, 2002
PICSS Results Homma et al., Circulation, 2002
PFO Closure Devices for Cryptogenic Stroke CLOSURE – Fulran et al., NEJM 2012 RESPECT – Carroll et al., TCT 2012 PC - Meier, et al., TCT 2012
PFO Closure in Cryptogenic Stroke: Conclusion There is no evidence for routine PFO closure in patients with cryptogenic stroke. We should continue to enroll patients in RCT trials to evaluate the effectiveness of endovascular PFO closure as a secondary stroke prevention strategy.