Download
1 / 1
10 likes | 164 Views
Procalcitonin-Guided Duration of Antimicrobial Therapy in Healthcare-Associated Pneumonia. Fatima Ali, Pharm.D. 1 , Jill Cwik, Pharm.D. 1 , Sarah M. Wieczorkiewicz, Pharm.D., BCPS 1 , and Robert Citronberg, MD, FIDSA 2

E N D
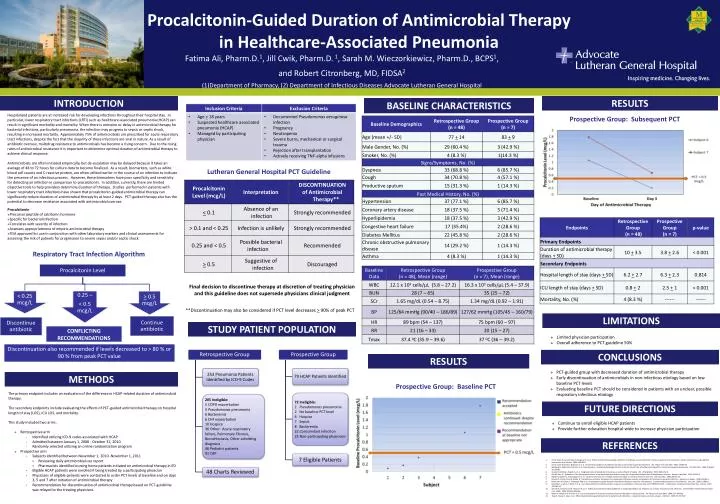
Procalcitonin-Guided Duration of Antimicrobial Therapy in Healthcare-Associated Pneumonia Fatima Ali, Pharm.D.1, Jill Cwik, Pharm.D. 1, Sarah M. Wieczorkiewicz, Pharm.D., BCPS1, and Robert Citronberg, MD, FIDSA2 (1)Department of Pharmacy, (2) Department of Infectious Diseases Advocate Lutheran General Hospital Discontinuation also recommended if levels decreased to > 80 % or 90 % from peak PCT value INTRODUCTION RESULTS BASELINE CHARACTERISTICS Continue antibiotic • Hospitalized patients are at increased risk for developing infections throughout their hospital stay. In particular, lower respiratory tract infections (LRTI) such as healthcare-associated pneumonia (HCAP) can result in significant morbidity and mortality. When there is omission or delay in antimicrobial therapy for bacterial infections, particularly pneumonia, the infection may progress to sepsis or septic shock, resulting in increased mortality. Approximately 75% of antimicrobials are prescribed for acute respiratory tract infections, despite the fact that the majority of these infections are viral in nature.As a result of antibiotic overuse, multidrug resistance to antimicrobials has become a rising concern. Due to the rising rates of antimicrobial resistance it is important to determine optimal duration of antimicrobial therapy to achieve clinical response. • Antimicrobials are often initiated empirically, but de-escalation may be delayed because it takes an average of 48 to 72 hours for culture data to become finalized. As a result, biomarkers, such as white blood cell counts and C-reactive protein, are often utilized earlier in the course of an infection to indicate the presence of an infectious process. However, these biomarkers have poor specificity and sensitivity for detecting an infection in comparison to procalcitonin. In addition, currently, there are limited objective tools to help providers determine duration of therapy. Studies performed in patients with lower respiratory tract infections have shown that procalcitonin-guided antimicrobial therapy can significantly reduce duration of antimicrobial therapy by at least 2 days. PCT-guided therapy also has the potential to decrease resistance associated with antimicrobial overuse. • Procalcitonin • Precursor peptide of calcitonin hormone • Specific for bacterial infection • Correlates with severity of infection • Assesses appropriateness of empiric antimicrobial therapy • FDA approved for use in conjunction with other laboratory markers and clinical assessments for assessing the risk of patients for progression to severe sepsis and/or septic shock Prospective Group: Subsequent PCT Lutheran General Hospital PCT Guideline Respiratory Tract Infection Algorithm Final decision to discontinue therapy at discretion of treating physician and this guideline does not supersede physicians clinical judgment **Discontinuation may also be considered if PCT level decreases > 90% of peak PCT LIMITATIONS STUDY PATIENT POPULATION CONFLICTING RECOMMENDATIONS • Limited physician participation • Overall adherence to PCT guideline 50% CONCLUSIONS RESULTS • PCT-guided group with decreased duration of antimicrobial therapy • Early discontinuation of antimicrobials in non-infectious etiology based on low baseline PCT levels • Evaluating baseline PCT should be considered in patients with an unclear, possible respiratory infectious etiology METHODS Prospective Group: Baseline PCT The primary endpoint includes an evaluation of the difference in HCAP-related duration of antimicrobial therapy. The secondary endpoints include evaluating the effects of PCT-guided antimicrobial therapy on hospital length of stay (LOS), ICU LOS, and mortality. This study included two arms: • Retrospective arm • Identified utilizing ICD-9 codes associated with HCAP • Admitted between January 1, 2008 - October 31, 2010 • Randomly selected utilizing an online randomization program • Prospective arm • Subjects identified between November 1, 2010 -November 1, 2011 • Reviewing daily antimicrobial use report • Pharmacists identified nursing home patients initiated on antimicrobial therapy in ED • Eligible HCAP patients were enrolled if being treated by a participating physician • Physicians of eligible patients were contacted to order PCT levels at baseline and on days 3, 5 and 7 after initiation of antimicrobial therapy • Recommendation for discontinuation of antimicrobial therapy based on PCT-guideline was relayed to the treating physicians FUTURE DIRECTIONS • Continue to enroll eligible HCAP patients • Provide further education hospital-wide to increase physician participation REFERENCES Christ-Crain M, Jaccard-Stolz D, Bingisser R, et al. Effect of procalcitonin-guided treatment on antibiotic use and outcome in lower respiratory tract infections: cluster-randomised, single-blinded intervention trial. Lancet. 2004; 363:600-7. Christ-Crain M, Stolz D, Bingisser R, et al. Procalcitonin guidance of antibiotic therapy in community-acquired pneumonia. Am J Respir Crit Care Med. 2006; 174:84-93. Spellberg B, Talbot GH, Brass EP, et al. Position paper: recommended design features of future clinical trials of antibacterial agents for community-acquired pneumonia. Clin Infect Dis. 2008; 47(Suppl 3):S249-65. Guven H, Altintop L, Baydin A, et al. Diagnostic value of procalcitonin levels as an early indicator of sepsis. Am J Emerg Med. 2002; 20(3):202-6. Kim KE, Han JY. Evaluation of the clinical performance of an automated procalcitonin assay for the quantitative detection of bloodstream infection. Korean J Lab Med. 2010; 30:153-9. Muller B, Becker KL, Schachinger H, et al. Calcitonin precursors are reliable markers of sepsis in a medical intensive care unit. Crit Care Med. 2000; 28(4):1-14. Schuetz P, Christ-Crain M, Muller B. Procalcitonin and other biomarkers for assessment of disease severity and guidance of treatment in bacterial infections. Advances in Sepsis. 2008; 6(3):82-9. Hochreiter M, Kohler T, Schweiger AM, et al. Procalcitonin to guide duration of antibiotic therapy in intensive care patients: a randomized prospective controlled trial. Crit Care. 2009; 13:R83-9. Bouadma L, Luyt CE, Tubach F, et al. Use of procalcitonin to reduce patients' exposure to antibiotics in intensive care units (PRORATA trial): a multicentre randomised controlled trial. Lancet. 2010; 375:463-74. Schuetz P, Christ-Crain M, Thomann R, et al. Effect of procalcitonin based guidelines vs standard guidelines on antibiotic use in lower respiratory tract infections: the ProHOSP randomized controlled trial. JAMA. 2009; 302(10):1059-66. Nobre V, Harbarth S, Graf JD, et al. Use of procalcitonin to shorten antibiotic treatment duration in septic patients. Am J Respir Crit Care Med. 2008; 177:498-505. Tang H, Huang T, Jing J, et al. Effect of procalcitonin-guided treatment in patients with infections: a systemic review and meta-analysis. Infection. 2009; 37:497-507.