Download
1 / 14
140 likes | 315 Views
Management of Chronic Heart Failure in Adults: Synopsis of the National Institute for Health and Clinical Excellence Guideline . Jonathan Mant , MD; abdallah al- mohammad , md ; Sharon Swain, BA, Phd ; and philippe laramee,dc,msc , for the guideline development group

E N D
Management of Chronic Heart Failure in Adults: Synopsis of the National Institute for Health and Clinical Excellence Guideline Jonathan Mant, MD; abdallah al-mohammad, md; Sharon Swain, BA, Phd; and philippelaramee,dc,msc, for the guideline development group Chris fontimayor ms-III Mercer University School of medicine Dr. Rahimi 9/9/2011
Heart Failure (HF) • A common clinical syndrome representing the end-stage of a number of different cardiac diseases • Result of any structural or functional cardiac disorder that impairs the ability of the ventricle to fill with or eject blood • Two types • Systolic Dysfunction • Diastolic Dysfunction
Heart Failure • Symptoms – dyspnea, orthopnea, paroxysmal nocturnal dyspnea, nocturnal cough, confusion and memory loss in advanced stages, diaphoresis and cool extremities at rest • New York Heart Association (NYHA) Classification • Class I – symptoms only with vigorous activities • Class II – symptoms with moderate exertion • Class III – symptoms with normal daily activities • Class IV – symptoms at rest
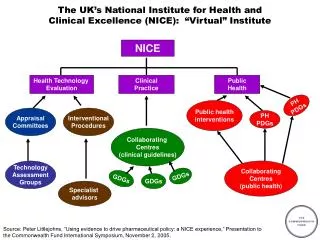
National Institute for Health and Clinical Excellence (NICE) • Develops clinical practice guidelines for the National Health Service of England and Wales • First guideline on HF in 2003 • Target population: Non-pregnant adults with symptoms of chronic HF • Exclusion: Patients with acute HF or acute exacerbations of chronic HF • Updated every 3 years • Literature searches for new evidence, warnings from licensing agencies , and major changes in costs • Actively seek out the views of health care professionals and patients
Guideline Development Process • Guideline development group (GDG)– general practitioners, specialist nurses, a consultant physician, consultant cardiologists, and 2 members representing patients and caregivers • Clinical question Literature review Evidence grading
High Quality Evidence for Pharmacologic Therapy • ACE inhibitors and ß-blockers reduce morbidity and increase survival in patients with left ventricular systolic dysfunction • No difference exists between selective ß-blockers (ie metoprolol) and nonselective ß-blockers (ie carvedilol) on the combined end point of mortality and hospitalization • Combination therapy of ARBs and ACE inhibitors increases risk of hyperkalemia • Adding ARB to ACE inhibitor and ß-blocker reduces the mortality and hospitalization caused by HF
Invasive Therapy Recommendations • Patients who are at any stage of HF with left ventricular systolic dysfunction should be considered for an implantable cardioverter-defibrillator (ICD) • Criteria • Sustained ventricular tachycardia or non-sustained ventricular tachycardia that is inducible on electrophysiology testing if the left ventricular ejection fraction (LVEF) is less than 35% • QRS of duration of 120 ms or longer if the LVEF is less than 30%
Rehabilitation • Moderate quality evidence shows that exercise rehab reduces hospital admissions for HF and increases long-term quality of life • GDG recommends supervised group exercise programs with psychological and educational components
Monitoring Patients With HF • Moderate quality evidence • Therapy guided by serum natriuretic peptide levels results in a reduction of hospitalizations due to HF • Therapy guided by serum natriuretic peptide levels reduces mortality in persons younger than 75 • Cost effective analysis demonstrated that serial serum natriuretic peptide monitoring was cost effective when used by specialists • Significant heterogeneity of evidence for the use of telemonitoring in decreasing hospitalizations • GDG has no recommendation for telemonitoring
New Evidence Since the Implementation of the 2010 NICE guideline • EMPHASIS-HF Study (Epleronone in Mild Patients Hospitalization and Survival Study in Heart Failure) • Significant reductions in hospitalization and mortality when epleronone therapy is started in patients hospitalized during the preceding 6 months or with persistent moderate elevation of serum natriuretic peptide levels (BNP≥250 ng/L) • SHIƒT (Systolic Heart Failure Treatment with the Iƒ Inhibitor Ivabradine Trial) • Ivabradine, Iƒ channel blocker in SA node, significantly reduces unplanned hospitalization and mortality in patients with HF due to left ventricular systolic dysfunction whose HR remains higher than 70bpm
Discussion • NICE guidelines are broadly consistent with other international guidelines (ESC and AHA) • Benefits • Earlier diagnosis • Better management • Decreased morbidity and mortality • Cost-effective