Download
1 / 29
290 likes | 416 Views
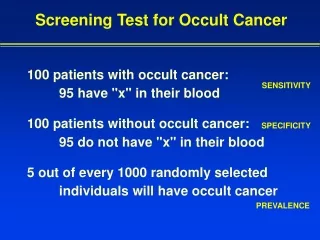
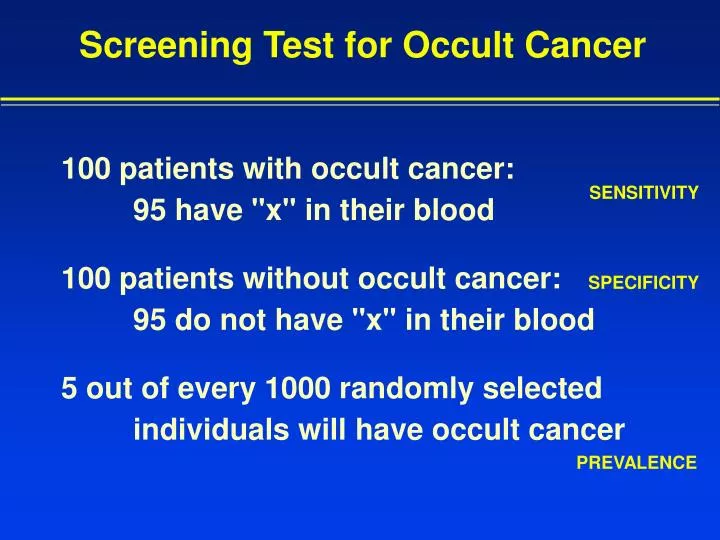
Screening Test for Occult Cancer. 100 patients with occult cancer: 95 have "x" in their blood 100 patients without occult cancer: 95 do not have "x" in their blood 5 out of every 1000 randomly selected individuals will have occult cancer. SENSITIVITY. SPECIFICITY. PREVALENCE.

E N D
Screening Test for Occult Cancer 100 patients with occult cancer: 95 have "x" in their blood 100 patients without occult cancer: 95 do not have "x" in their blood 5 out of every 1000 randomly selected individuals will have occult cancer SENSITIVITY SPECIFICITY PREVALENCE
"x" present "x" absent Occult Cancer Present 475 25 500 Occult Cancer Absent 4,975 94,525 99,500 5,450 94,550 2 X 2 Table 100,000 If a patient has “x” in his blood, chance of occult canceris 475 / 5450 = 8.7%
Test negative Test positive Disease Present TP + FN Disease Absent FP + TN TP + FP FN + TN Standard Terminology True Positives (TP’s) False Negatives (FN’s) False Positives (FP’s) True Negatives (TN’s) Entire Population
Positive Predictive Value Formula (Sens)(Prev) PV+ = (Sens)(Prev) + (1-Spec)(1-Prev)
Detection of Prostatic Cancer by Solid-Phase Radioimmunoassay of Serum Prostatic Acid Phosphatase
Editorial “The clear implication of the accompanying report is that mass screening on the basis of a blood test alone can reverse this gloomy experience [of fatal delays in diagnosis of prostate cancer].” New England Journal of Medicine December 22, 1977
Medical Journal Advertisement to Physicians Posed by a Professional Model
Advertisement “(You should be aware of) a new blood test called the Male-P.A.P. test ... a new, more sensitive method that your physician can use to detect chemical signals of a cancerous growth in the prostate. ... And even though all lab tests must be ordered by a physician, we believe that you should know the facts.” New York Times, January 21, 1979
Sensitivity # of patients # of positive tests sensitivity Patients with prostate 113 79 70%cancer Stage I 24 8 33% Stage II 33 26 79% Stage III 31 22 71% Stage IV 25 23 92%
Specificity # of patients # of positive tests specificity Patients without prostate 217 13 94%cancer Normal controls 50 0 BPH 36 2 After total prosta- 28 1 tectomy Other cancers 83 9 Misc. GI disorders 20 1
Use As Screening Test • Without rectal examination: • Sensitivity = 70% Specificity = 94% • Prevalence 33/100,000 • PV+ = 0.41% (i.e., 1 in 244 subjects) • With rectal examination: • Sensitivity = 33% Specificity = 94% • Prevalence 33/100,000 • PV+ = 0.19% (i.e., 1 in 526 subjects)
When is the test useful for screening? Suppose patient has a nodule on rectal examination: • Sensitivity (Stage 2 of disease) = 79% • Specificity = 94% • Prevalence = 50% !! PV+ = 93% (chance of cancer if acid phosphatase is positive) PV- = 82% (chance that there is no cancer if acid phosphatase is negative)
Predictive Values in Patients with a Nodule PAP+ 93% 50% PAP- 18%
Combining Tests For Screening: If a prostate biopsy is now performed, it needs to be considered as another test. Specificity = 100% Sensitivity depends on talent and statistics of surgeon doing the procedure Prevalence is 50% if acid phosphatase has not been measured, but is 93% if acid phosphatase is positive and 18% if acid phosphatase is negative.
Sequential Testing BX+ 100% PAP+ 93% 50% BX+ 100% PAP- 18%
Chance of Cancer after Negative Biopsy Sensitivity of Biopsy 50% 87% 10% 70% 80% 6% 90% 56% 2% Acid Phosphatase positive (93% chance before biopsy) Acid Phosphatase negative (18% chance before biopsy)
Sequential Testing BX+ 100% PAP+ 93% BX- 56% 50% BX+ 100% PAP- 18% BX- < 2%
Typical Assumptions with theUse of Bayes' Theorem • Completeness (for example, all men either have or do not have prostate cancer; there are no other possibilities) • Mutual exclusivity (for example, if a man has prostate cancer, he cannot simultaneously NOT have prostate cancer) • Conditional independence (for example, acid phosphatase and a biopsy result ARE conditionally independent tests; rectal exams and acid phosphatase may NOT be conditionally independent)
References Foti et al. “Detection of prostate cancer by solid-phase radioimmunoassay of serum prostatic acid phosphatase.” New England Journal of Medicine 297:1357-1361 (1977) Watson, R.A. and Tang, D.B. “The predictive value of prostatic acid phosphatase as a screening test for prostatic cancer.” New England Journal of Medicine 303:497-499 (1980) Berwick, D.M., Fineberg, H.V., and Weinstein, M.C. “When doctors meet numbers.” American Journal of Medicine 71:991 (1981)
What is a “Positive Test”? • All the analysis has assumed that it is clear whether a test is positive or negative • In reality, many tests involve continuous values so that one result may be “more positive” than another • How should one define the cut-off at which a test is judged to be abnormal?
Normal True Negatives “Normal” cutoff False Positives False Negatives True Positives Diseased Continuously Valued Variables Result
Normal Diseased Continuously Valued Variables • Fewer false positives (more “conservative”) • More false negatives • Higher specificity • Lower sensitivity “Normal” cutoff Result
Normal “Normal” cutoff Diseased Continuously Valued Variables Result • Fewer false negatives (more “aggressive”) • More false positives • Higher sensitivity • Lower specificity
Receiver Operating Characteristic(ROC) Curves Test B Test A ROC curve shifts to left, indicating the new test (B) is “better” – or a better indicator to disease presence (more discriminatory). True Positive Rate = Sensitivity False Positive Rate = 1 - Specificity
The Importance of the Gold Standard • Evaluating the value of a new test requires having some other method for determining “truth” • Methods for determining truth are called gold standards • Gold standards are often expensive, time consuming, uncomfortable, or risky • Biopsies • Major invasive procedures or surgery • Autopsies • Integrated opinions of “super experts” • We often seek simple, inexpensive, rapid, and safe tests that can perform almost as well as the gold standard