Download
1 / 61
2.26k likes | 15.07k Views
THORACIC INCISIONS. PRESENTER: DR ANEFU, N. E MODERATOR:DR S. EDAIGBINI AHMADU BELLO UNIVERSITY TEACHING HOSPITAL,ZARIA,NIGERIA . OUTLINE. INTRODUCTION HISTORICAL PERSPECTIVES ANATOMY OF THE CHEST BASIS GENERAL PRINCIPLE TYPES OF THORACIC INCISIONS CURRENT TREND FUTURE TREND

E N D
THORACIC INCISIONS PRESENTER: DR ANEFU, N. E MODERATOR:DR S. EDAIGBINI AHMADU BELLO UNIVERSITY TEACHING HOSPITAL,ZARIA,NIGERIA
OUTLINE • INTRODUCTION • HISTORICAL PERSPECTIVES • ANATOMY OF THE CHEST • BASIS • GENERAL PRINCIPLE • TYPES OF THORACIC INCISIONS • CURRENT TREND • FUTURE TREND • CONCLUTION
INTRODUCTION • Incision;- Is a surgical wound made by a surgeon on the skin, with intension of gaining access to a lesion beneath or cavity. • Such wounds created anywhere on the chest (thoracic) wall is thoracic incision
Historical perspective • Development evolution thoracic incision is closely related to the development of thoracic surgery • Used in ancient time for draining abscesses in the chest
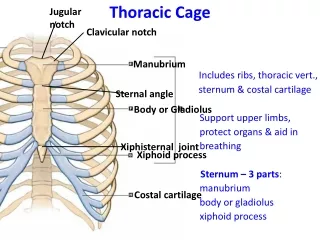
CHEST WALL • Bony rib cage;- manubrum, sternum, 12 pair of rib, coastal cartilage & thoracic vertebrae • Soft tissue covering:- muscles, neurovascular bundles, other connective tissues • Two aperture • Superior=root of the neck • Inferiorly=separated from abdominal cavity by diaphragm
In spite of the large intra-thoracic space, separate pleural spaces &rigid- ribbed chest wall, its anatomy makes specific incision selection crucial to the ease & safety of a given thoracic procedure • Respiration is still possible; due to the nature of the joint & muscular attachments
General principles • Patient evaluation & clinical assessment • History, P.E, Lab & Radiological investigations-LFT, Spirometric measurement,SPO2,CXR, • Performance score rating • Patient education/counseling/consent • Start Chest physiotherapy • Peri-op monitoring/medications
Gen. principles • Anaesthesia(G.A,double lumen ETT or single lung intubation) • Analgesia( epidural catheters,intercostal nerve block) • Surgery • Antibiotics prophylaxis • Follow-up
Analgesia CTU-ABUTH • Taken very seriously • Intra-op =I.V pentazoxine • Post-op =Triple px • Opioid; pentazoxine • NSAIDs;diclofenac • Acetaminophen;PCM
Prophylactic Antibiotics-CTU • Intra-op =3rd generation cephalosporin e.gceftriaxone + metronidazole, repeated after 8hrs, • Post-op =same extended X 2-3/7
Surgical principles • To allow a successful surgical outcome • Adequate exposure • Preserve chest-wall function & appearance • Incision along langers line or positioned to minimize visibility • Closure-rigid approximation & strict layered closure
Optimal approach depends on Bony anatomy Location & extent of pathology Location of the hilum Objective of the procedure Chest drainage
Types of thoracic incisions • Sternotomy • Thoracotomy • Axillarythoracotomy • Anterior mediastinotomy • Thoracoabdominal incision
Types cont… • Bilateral Trans-sternalthoracotomy( clam-shell incision) • Extra-thoracic approaches to the thorax
Sternotomy incisions • Partial • Hemisternotomy (spares 6-8cm skin) • Complete • Suprasternalnotchxyphoid process • Cosmetically appealing type of incision e.ginframammary (bikini type) incision
Median sternotomy Indications exposure of ant. & middle mediast lower cervical procedures Tracheal resection& reconstruction
Indications • Excision of thyroid masses & parathyroid adenomas • Excision of cervical oesophagealtumours • Exposure of heart & great vessels • In cardiopulmonary bypass
Advantages • Quick to perform • Excellent exposure • Safe • Heals quickly • Less incisional pain
Disadvantages • Many finds the vertical incision unsighty • Gives limited exposure of the lower chest & posterior mediastinum • May lead to post-op complications-unsteable sternum, infections
Technique • Standard sternotomy • Open sternotomy • Re-operative sternotomy • Partial sternal split
Less invasive sternotomy incisions • Hemisternotomy- suprasternalnotch,tee-off to the R at interspace 4 or xyphoid,tee-off,R, at interspace 2 • Full sternotomy with skin sparing • Bikini-type (inframammary) incision- cosmesis
Post-op care • ICU MANAGEMENT/MONITORING • O2 DELIVERY VIA NEBULIZER • PAIN MANAGEMENT( I.Vanalgesics,Eidural nr block) • PHYSIOTHERAPY
COMPLICATIONS • Anaesthetic:- arrhythmias, laryngeal spasm Specific :- Early; haemorrhage,injury to contiguous structures, pneumothorax, haemothorax, Late; infection, empyemathoracis, post surgery pain
Complications • Mediastinitis (S.aureu31%,E.coli3%,enterococcus 2%) • Sternalosteomyelitis • Brachial plexus injury,incidence:1.4-6.5%
Thoracotomy • Standard thoracotomy incisions • Defined arbitrarily in relation to the position of Latissismusdorsi muscle,which is laterally sited on the chest wall
Types of thoracotomy incisions • Lateral • Anterior • Anterolateral • Posterolateral • Posterior • others
Indications for posterolateral incision • Standard thoracotomy incisions can be used for a wide range of surgical procedures involving; • The Heart • Oesophagus • Mediastinum • Ipsilateral lung
Advantages • Flexibility of the incision • Wide range of intra-thoracic exposure • Proven experience with these incisions has made them the standard thoracic incisional approach
Disadvantages • Has potential for poor exposure , if wrong interspace is chosen • Unilateral hemithorax exposure • Incisional pain • Disability related to division of chest wall muscles • Detrimental effect on pulmonary function
Technique (posterolateral) • Induction using single/double lumen tube • Appropriate monitoring • Anaesthesia-G.A+ETT • Positioning –lateral decubitus position • Cleaning/drapping
Crescent or “lazy-S”incision, transversely • Dissected down & scapular retracted • Pleural space entered • Pleural/mediastinal drainage • Thoracotomy closure
Option for entering the pleural space after posterolateralthoracotomy
Intercostal approach-incising i.c muscles • Utilizing intercostal incision but to divide one or more ribs • To resect a rib, enter through its periosteal bed
Anterior & anterolateralthoracotomy • Indications • Has greater use historically • Used for pulmonary resection • Cardiac procedures • Management of mediastinal masses • Oesophageal pathology
Technique • Monittoring • Anaesthesia are same as posterolatral • Supine position • Chest elevated at 30-45 • Curved submammary incision, extended laterally(anterolateral)
Lateral thoracotomy • Within confines of latissimusdorsi • Transverse incision • 1-2cm inferior to the scapular
Complications • Post thoracotomy incision pain • Wound infection • Wound dehiscence • Bronchopleural fistula-8% • Empyema thoracis-2.2%
Muscle-sparing thoracotomy • Indications • As in std thoracotomy • Variant of std thoracotomy • Well established • Has less complications
Advantages • Less early post-op pains • Greater shoulder girdle strength • Most result in quick closure • Preserve chest wall muscle • Prevent chest wall deformity
Axillarythoracotomy • Indications • 1st rib disection • Apical bleb Dx • Mgt of spontaneous pneumothorax with apical pleurectomy or pleurodesis • Staging of lung cancer
Patient positioning & incision for a vertical axillary incision