Download
1 / 1
10 likes | 148 Views
Abnormal attachment beyond delivery – Placenta increta. . Ragupathy K, Dina O, Gerghis H Doncaster Royal Infirmary.

E N D
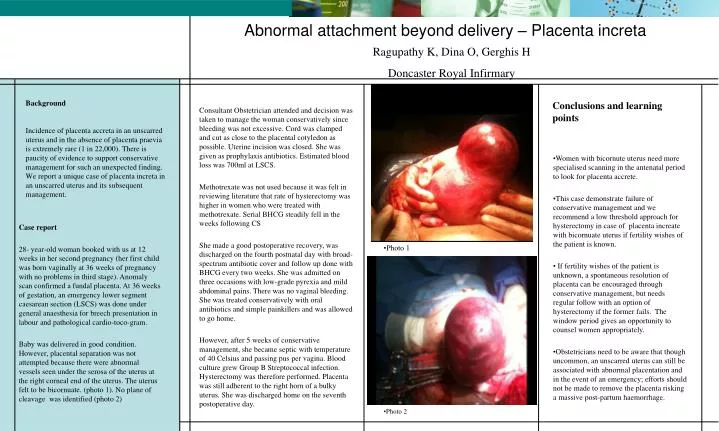
Abnormal attachment beyond delivery – Placenta increta  Ragupathy K, Dina O, Gerghis H Doncaster Royal Infirmary Consultant Obstetrician attended and decision was taken to manage the woman conservatively since bleeding was not excessive. Cord was clamped and cut as close to the placental cotyledon as possible. Uterine incision was closed. She was given as prophylaxis antibiotics. Estimated blood loss was 700ml at LSCS. Methotrexate was not used because it was felt in reviewing literature that rate of hysterectomy was higher in women who were treated with methotrexate. Serial BHCG steadily fell in the weeks following CS She made a good postoperative recovery, was discharged on the fourth postnatal day with broad-spectrum antibiotic cover and follow up done with BHCG every two weeks. She was admitted on three occasions with low-grade pyrexia and mild abdominal pains. There was no vaginal bleeding. She was treated conservatively with oral antibiotics and simple painkillers and was allowed to go home. However, after 5 weeks of conservative management, she became septic with temperature of 40 Celsius and passing pus per vagina. Blood culture grew Group B Streptococcal infection. Hysterectomy was therefore performed. Placenta was still adherent to the right horn of a bulky uterus. She was discharged home on the seventh postoperative day. Conclusions and learning points Background Incidence of placenta accreta in an unscarred uterus and in the absence of placenta praevia is extremely rare (1 in 22,000). There is paucity of evidence to support conservative management for such an unexpected finding. We report a unique case of placenta increta in an unscarred uterus and its subsequent management. Women with bicornute uterus need more specialised scanning in the antenatal period to look for placenta accrete. This case demonstrate failure of conservative management and we recommend a low threshold approach for hysterectomy in case of placenta increate with bicornuate uterus if fertility wishes of the patient is known. If fertility wishes of the patient is unknown, a spontaneous resolution of placenta can be encouraged through conservative management, but needs regular follow with an option of hysterectomy if the former fails. The window period gives an opportunity to counsel women appropriately. Obstetricians need to be aware that though uncommon, an unscarred uterus can still be associated with abnormal placentation and in the event of an emergency; efforts should not be made to remove the placenta risking a massive post-partum haemorrhage. Case report 28- year-old woman booked with us at 12 weeks in her second pregnancy (her first child was born vaginally at 36 weeks of pregnancy with no problems in third stage). Anomaly scan confirmed a fundal placenta. At 36 weeks of gestation, an emergency lower segment caesarean section (LSCS) was done under general anaesthesia for breech presentation in labour and pathological cardio-toco-gram. Baby was delivered in good condition. However, placental separation was not attempted because there were abnormal vessels seen under the serosa of the uterus at the right corneal end of the uterus. The uterus felt to be bicornuate. (photo 1). No plane of cleavage was identified (photo 2) Photo 1 Photo 2