Download
1 / 2
20 likes | 222 Views
Resistance to passage of ETT:use ½ size smaller Cuff pressure to be kept < 20 cm H2O Leak at <10cm H2O: exchange ETT for ½ size larger Smaller ETT= Raw ETT follows chin. Pt position for care and CXR ++ important. Chin low=ETT low

E N D
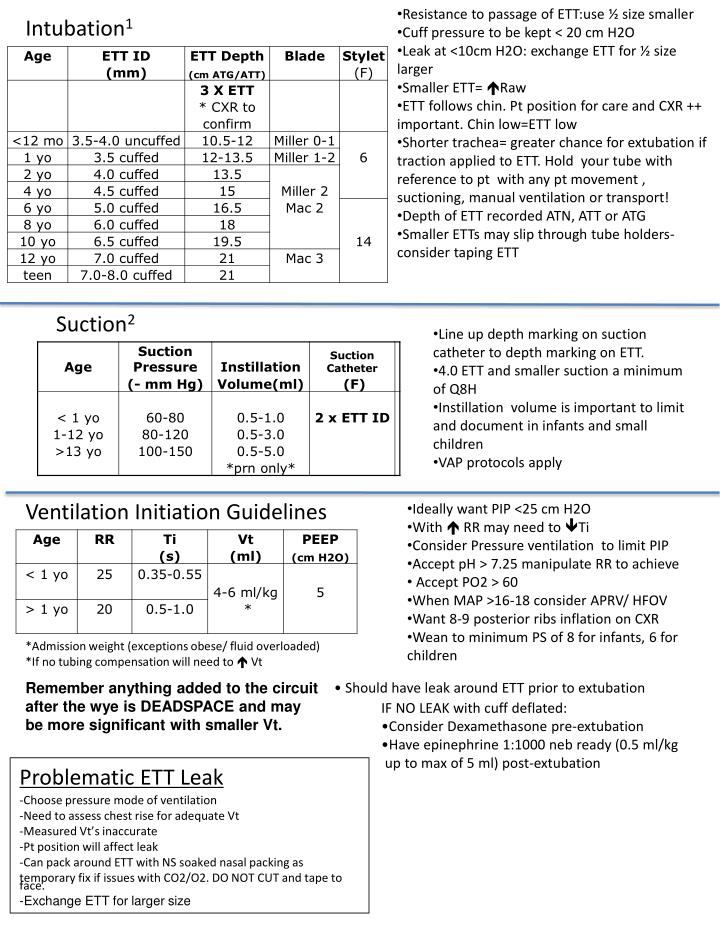
Resistance to passage of ETT:use ½ size smaller • Cuff pressure to be kept < 20 cm H2O • Leak at <10cm H2O: exchange ETT for ½ size larger • Smaller ETT= Raw • ETT follows chin. Pt position for care and CXR ++ important. Chin low=ETT low • Shorter trachea= greater chance for extubation if traction applied to ETT. Hold your tube with reference to pt with any pt movement , suctioning, manual ventilation or transport! • Depth of ETT recorded ATN, ATT or ATG • Smaller ETTs may slip through tube holders- consider taping ETT Intubation1 Suction2 • Line up depth marking on suction catheter to depth marking on ETT. • 4.0 ETT and smaller suction a minimum of Q8H • Instillation volume is important to limit and document in infants and small children • VAP protocols apply Ventilation Initiation Guidelines • Ideally want PIP <25 cm H2O • With RR may need to Ti • Consider Pressure ventilation to limit PIP • Accept pH > 7.25 manipulate RR to achieve • Accept PO2 > 60 • When MAP >16-18 consider APRV/ HFOV • Want 8-9 posterior ribs inflation on CXR • Wean to minimum PS of 8 for infants, 6 for children *Admission weight (exceptions obese/ fluid overloaded) *If no tubing compensation will need to Vt • Should have leak around ETT prior to extubation • IF NO LEAK with cuff deflated: • Consider Dexamethasone pre-extubation • Have epinephrine 1:1000 neb ready (0.5 ml/kg • up to max of 5 ml) post-extubation Remember anything added to the circuit after the wye is DEADSPACE and may be more significant with smaller Vt. • Problematic ETT Leak • Choose pressure mode of ventilation • Need to assess chest rise for adequate Vt • Measured Vt’s inaccurate • Pt position will affect leak • Can pack around ETT with NS soaked nasal packing as • temporary fix if issues with CO2/O2. DO NOT CUT and tape to face. • -Exchange ETT for larger size
*Lower limit of SBP • =70 + (2 x age in years) • Infants and small children don’t like strangers. RR, BP and HR will . Evaluate prior to entering room if possible • Respiratory failure is 1° cause of cardiac collapse. Intervene early. • Children have large compensation capacity. Must recognize shock early. Too late once decompensated. Normal Vital Signs1 Signs of WOB • ↑RR, Apnea • Nasal flaring • Head bobbing • Seesaw respirations • Chest retractions • Tracheal tug • Accessory muscle use • grunting CPR Guidelines1 Airway/anatomy differences (adult pattern by ~8 years of age)