Download
1 / 18
320 likes | 1.81k Views
Syndrome of Inappropriate Antidiuretic Hormone (SIADH). Objectives. The learner will be able to: Describe the pathophysiology of SIADH. Identify appropriate clinical management of SIADH. Description.

E N D
Objectives The learner will be able to: • Describe the pathophysiology of SIADH. • Identify appropriate clinical management of SIADH.
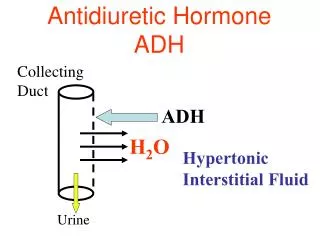
Description • Inappropriate secretion of antidiuretic hormone, inappropriate for feedback mechanisms, leading to fluid and electrolyte disturbances • Kidneys absorb free water, despite normal blood volume and intravascular osmolality, resulting in low sodium levels (hyponatremia) and concentrated urine output.
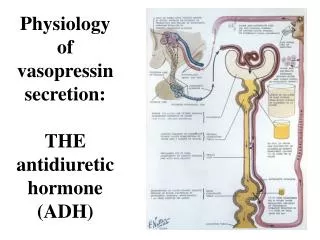
Normal Secretion of ADH • Regulated by receptors in the kidneys, heart, and hypothalamus in response to: • Elevated serum osmolality • Low blood pressure or volume
Inappropriate ADH Secretion • Malignancy • Central nervous system disorders • Pulmonary disease • Stress/pain • Dehydration
Risk Related to Malignancy • Lung cancer • Small cell lung cancer (80%) • Primary brain tumors • Other • Pancreas • Duodenum/colon • Bladder/prostate
Other Risks • Advanced age • Tobacco use • Medications • Opioids • Antidepressants • NSAIDs • Anesthetics
Significance • Hyponatremia • Seizures • Coma • Death
Symptoms • Mild hyponatremia (125134 mEq/L) • Thirst • Anorexia • Nausea • Headache • Muscle cramps or weakness
Symptoms (cont.) • Moderate hyponatremia (115124 mEq/L) • Weight gain • Oliguria • Increasing neurologic manifestations
Symptoms (cont.) • Severe hyponatremia (<115 mEq/L) • Papilledema • Delirium • Hypoactive reflexes • Ataxia
Diagnosis • Low serum sodium (<135 mEq/L) • Low serum osmolality (<275 mOsm/kg) • Low BUN • Elevated urine sodium (>220 mEq/24 hrs) • Elevated urine osmolality (>1,200 mOsm/kg water • Elevated urine specific gravity (>1.032)
Treatment • Treat underlying malignancy. • Free water restriction (5001,000 ml/day) • Discontinue problematic drug therapy. • Pharmacologic inhibition of ADH • Demeclocycline • Lithium • Hypertonic saline (3%5%)
Goals of Therapy • Slow adjustment of sodium level • 125130 mEq/L • Avoid fluid overload. • Minimize hypotonic solutions. • Add furosemide with hypertonic therapies. • Prevent central pontine myelinolysis.
Nursing Management • Early recognition of risk • Monitor intake/output and weight. • Monitor electrolytes (sodium). • Monitor mental status. • Monitor neurologic signs. • Provide client and family education.
Dealing With Fluid Restriction • Space fluids evenly throughout the day. • Include high-sodium fluids. • Broth, tomato/orange juice, and milk • Perform oral care q two to four hours. • Use artificial saliva or oral moisturizers. • Suggest sugarless gum/candy. • Avoid alcohol mouthwashes or nicotine products.
References Clancey, J.K. (2006). Syndrome of inappropriate antidiuretic hormone secretion. In M. Kaplan (Ed.),Understanding and managing oncologic emergencies: A resource for nurses (pp. 197217). Pittsburgh, PA: Oncology Nursing Society. Flounders, J.A. (2003). Syndrome of inappropriate antidiuretic hormone [Online exclusive]. Oncology Nursing Forum, 30, E36E68. Fojo, A.T. (2005). Metabolic emergencies. In V.T. DeVita, S. Hellman, & S.A. Rosenberg (Eds.), Cancer: Principles and practice of oncology (7th ed., pp. 22922300). Philadelphia, PA: Lippincott Williams and Wilkins. Gobel, B.H. (2005). Metabolic emergencies. In J.K. Itano & K.N. Taoka (Eds.), Core curriculum for oncology nursing (4th ed., pp. 383421). St. Louis, MO: Elsevier Saunders. Keenan, A.K. (2005). Syndrome of inappropriate antidiuretic hormone. In C.H. Yarbro, M.H. Frogge, & M. Goodman (Eds.), Cancer nursing: Principles and practice (6th ed., pp. 940945). Sudbury, MA: Jones and Bartlett.
References (cont.) Langfeldt, L.A. (2003). Syndrome of inappropriate antidiuretic hormone secretion in malignancy: Review and implications for nursing management. Clinical Journal of Oncology Nursing, 7, 425430. Moore, J.M. (1998). Syndrome of inappropriate antidiuretic hormone. In B.L. Johnson & J. Gross (Eds.), Handbook of oncology nursing (3rd ed., pp. 711721). Sudbury, MA: Jones and Bartlett. Richerson, M.T. (2004). Electrolyte imbalances. In C.H. Yarbro, M.H. Frogge, & M. Goodman (Eds.), Cancer symptom management (3rd ed., pp. 440453). Sudbury, MA: Jones and Bartlett. Terpstra, T.L., & Terpstra, T.L. (2000). Syndrome of inappropriate antiduiretic hormone secretion: Recognition and management. MEDSURG Nursing, 9, 6168.