Download

1 / 56
670 likes | 1.09k Views
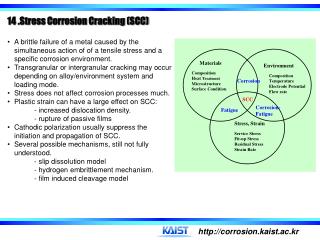
Compassion Fatigue: What’s New? What Works?. Françoise Mathieu, M.Ed., CCC. Certified Canadian Counsellor & Compassion Fatigue Specialist. www.compassionfatigue.ca. •Background: Robin Cameron. www.compassionfatigue.ca. My amazing team. Diana Tikasz, MSW RSW Hamilton.

E N D
Compassion Fatigue: What’s New? What Works? Françoise Mathieu, M.Ed., CCC. Certified Canadian Counsellor & Compassion Fatigue Specialist www.compassionfatigue.ca
My amazing team Diana Tikasz, MSW RSW Hamilton Rebecca Brown, MSW RSW London Lori Tomalty-Nusca, ECE Burlington Meaghan Welfare, BA Kingston
Ten Years On… •Walking the Walk CF workshop has been offered to thousands of Canadians across the country •Nurses, social workers, MH counsellors, PSWs, teachers, physicians, allied health professionals, victim service workers, court reporters, lawyers, judges, ministers, chaplains, police officers, paramedics, prison staff, alzheimers societies, palliative care… •Approx 300 CF Educators trained through Train the Trainer program •Various organizations implementing CF education as part of their staff wellness plan (Peel Region, York Region, Bruyere Continuing Care, Yukon and NWT Victim Services, to name a few). •Now: more attention being given to organizational health and how agencies can help reduce/prevent CF-VT
The Current Reality… •Deeply compromised system •Ongoing challenges and cutbacks •Difficult stories •Increasingly complex cases (even in schools, end of life care…) •Big org health assessment – interviewed all staff individually. What came out? Who coped well and who didn’t? • Those who struggled the most were: those who did not have an external practice of some kind to manage their stress, people who were angry and resentful and held on to it.
The Compassion Fatigue Workbook Published by Routledge - December 2011
The expectation that we can be immersed in suffering and loss daily and not be touched by it is as unrealistic as expecting to be able to walk through water without getting wet. Remen, 1996
Definitions • Compassion Fatigue • Vicarious Trauma • Moral Distress • Burnout • Chronic stress
Compassion Fatigue •A profound and gradual emotional and physical exhaustion that helping professionals and caregivers can develop over the course of their career. •An erosion of all the things that keep us connected to others in our caregiver role: our empathy, our hope, our ability to tolerate strong emotions/difficult stories in others, and of course our compassion - not only for others but also for ourselves. •Changes in our personal and professional lives: we become dispirited and increasingly bitter at work, contribute to a toxic work environment, more prone to clinical errors, violate client boundaries, lose a respectful stance towards our clients. short-tempered with our loved ones and feel constant guilt or resentment at the never ending demands on our personal time. •Can also happen to caregivers (“caregiver fatigue”)
Vicarious Trauma •Repeated exposure to difficult stories changes our view of the world. •Can cause nightmares, difficulty getting rid of certain images, an intense preoccupation with a particular story or event we’ve been exposed to. •”When external trauma becomes internal reality” Lipsky 2009 “Impacts the entire nervous system” •Can happen through work (stories we are told or stories we read) and through media exposure. •Accumulates over time & across clients. •Both CF and VT are occupational Hazards
What happens to the stories you hear at work? • What are your particular vulnerabilities? • How do you protect yourself while doing this very challenging work? • Were you trained for this?
Primary vs Secondary Trauma • Secondary Trauma: “Trauma reactions that involve other’s trauma imagery or trauma stories” characterized by “panic, horror or helplessness in relation to the event” (Tikasz) • Primary Trauma: • As a consequence of the work: e.g. EMS – car accidents, fatalities involving children • From our personal lives, our own past • Post Traumatic Stress Disorder (PTSD)
Moral Distress “[…] happens when there are inconsistencies between a [helper’s] beliefs and his or her actions in practice” (Baylis 2000) • “when policies or routines conflict with […] beliefs about […] patient care” (Mitchell 2000)
Burnout • “Physical & emotional exhaustion as a result of prolonged stress and frustration” • Depleted ability to cope with work demands • Sense of powerlessness to achieve goals • Does not necessarily alter our view of the world, but our view of the workplace • Can happen in any occupation
Occupational Hazards • We don’t get CF/VT because we screwed up, we get it because we care • Vicarious Trauma is a natural consequence of trauma exposure
Primary Trauma Compassion Fatigue Vicarious & Secondary Trauma Burnout
Current ResearchTerminology - A need for more clarity • Beth Stamm: "The controversy regarding secondary trauma is not its existence but what it should be called.” • Nadine Najjar et al 2009 review of all the research to date on compassion fatigue in cancer-care providers • Conclusion: there still exists "an ambiguous definition of compassion fatigue that fails to adequately differentiate it from related constructs (e.g. burnout, secondary traumatic stress)." • We are working on getting a set of working definitions we all agree on, but we're not there yet. Stamm (1995) Najjar, Nadine et al (2009) Journal of Health Psychology, Vol 14(2) 267-277.
Some recent data •Depending on the studies, 40-85% of health care professionals were found to have CF and/or high rates of STS •57% of SW have been threatened, 16 % physically assaulted •40% of nurses physically assaulted •52% military chaplains at medium to high risk for anxiety and depressive disorders - this is twice as high as the norm for CF members and higher than general population
Some recent data 2009 AMA study of junior doctors •54% met the criteria for CF •69% met the criteria for burnout •71% had lower than average levels of job satisfaction Markwell & Wainer, Doctors’ Health, MJA Vol 191, No 8, 19 Oct 2009
Data con’t •2005 survey of the health of nurses (Canada): 8/10 nurses had accessed their EAP which is over twice as high as the EAP use by the total employed population •DV lawyers: significantly higher levels of STS and burnout compared to other mental health providers •2011 study of US surgeons had thought about suicide 1.5-3 times more than the general population. Only 26% of them had sought psychological help for their SI. •US immigration judges higher levels of burnout than hospital physicians and prison wardens •59% of MH professionals are willing to seek help vs 15% of law enforcement professionals
Green Cross Standards of Self Care Guidelines First, do no harm to yourself in the line of duty when helping/treating others Second, attend to your physical, social, emotional and spiritual needs as a way of ensuring high quality services for those who look to you for support as a human being
What Works?7 steps individuals (and organizations) can take to reduce CF/VT
What Works? 1) SOCIAL SUPPORT IN THE WORKPLACE "the most significant factor associated with compassion satisfaction” (Killian 2008 study of trauma counsellors) 2) TRAINING ON SELF CARE AND SELF AWARENESS "[...] most of the therapists interviewed observed that they had not had any courses or specific training on professional self-care, and this was an important but neglected area in training.” Killian 2008 • Killian recommends that self awareness and self care become integral parts of the curriculum for all helping professionals. Killian, K.D. Helping Till it Hurts? A Multimethod Study of Compassion Fatigue, Burnout, and Self-Care in Clinicians Working With Trauma Survivors in Traumatology, Vol 14, No 2, June 2008.
Step Two: Self Awareness Psychoneuroimmunology Dr Gabor Maté
Step Two: Self Awareness con’t Long term effects of chronic stress •“Our immune system does not exist in isolation from daily experience.” (Maté, 2003, p.6)
Step Two: Self Awareness con’t • Chronic stress: “chronically high cortisol levels destroy tissue. Chronically elevated adrenalin levels raise the blood pressure and damage the heart.” (Maté, 2003 p.35) • See p 35 for alzheimer’s disease eg.
Step Two: Self Awareness con’t The “Gut” Feeling • “[…] we have lost touch with the gut feelings designed to be our warning system. […] We keep ourselves in physiologically stressful situations, with only a dim awareness of distress or no awareness at all.” Maté, 2003 p36
Self Awareness: a Key Strategy for CF/VT • Being aware of our current feelings, actions and reactions • Gaining an understanding and an awareness of how we deal with anger, hurt and resentment • Being aware of the dynamics from our past that influence the every day choices we make: Why did you choose to go into this field and not another? Did you pick this profession because of a trauma or loss you experienced in your own life? Were you already a helper in your family of origin? Are you the go-to person in your personal life? Do you feel empty or unimportant unless you are in a helping role? • Understanding how your own childhood history affects your reactions to your clients’ stories (countertransference) • Being in tune with your stress signals: Do you have a good sense of how your body communicates to you when it is overwhelmed? Do you get sick as soon as you go on vacation, develop hives, get a migraine when you are stressed? Many of us live in state of permanent overload and are dimly aware of it. What happens when you feel angry? Do you explode or do you swallow your rage? Where in your body do you feel your anger? • Are you aware of the ways in which you sabotage your self care? (by saying yes to requests you don’t have time for, by taking on more responsibilities, by drinking excessively, by cancelling a therapy appointment…)
Step Two: Self Awareness con’t Jon Kabat Zinn – Mindfulness Stress Reduction “Stress Reduction in 6 parts” Video on Youtube
Mindfulness-Based Stress Reduction • Article on website www.compassionfatigue.ca • Book: Full Catastrophe Living by John Kabat-Zinn
Mindfulness Stress Reduction •Research on the effectiveness of MBSR is highly conclusive: over 25 year of studies clearly demonstrate that MBSR is helpful in reducing emotional distress and managing severe physical pain. •MBSR has been used successfully with patients suffering from chronic pain, depression, sleep disorders, cancer-related pain and high blood pressure. (Cohen-Katz et al, 2005) •Based at Toronto's CAMH, Zindel Segal has developed a mindfulness-based cognitive therapy program for treating depression that has shown to be highly effective •MBSR and Compassion Fatigue: www.compassionfatigue.ca
3) Rebalancing Caseload & Workload Reduction"To combat compassion fatigue and burnout, agency administrators and therapists may also wish to ask themselves "How many cases are too many? ” Killian, 2008 What works? Con’t
What works? Con’t 4) Limiting Trauma Inputs •Limiting media exposure/traumatic stories •Low Impact Debriefing aka “sliming” see my website for an article describing this process: www.compassionfatigue.ca “resources”
Step Four con’t - Limiting Trauma Inputs Low Impact Debriefing • Increased Self Awareness • Fair Warning • 3) Consent • 4) Low Impact Disclosure
What works? Con’t 5) Improved Work/Life Balance 2009 Duxbury report on role overload in health care: • 3/5 health care workers suffering from role overload • 36% report high levels of depressed mood • 1 in 4 employee was planning on leaving their job at the hospital - not for higher pay, but for “greater control over work hours and more respect”
Step Five Con’t Take Time for Your LifeCheryl Richardson • The best Work-Life balance resource available
RelationshipsEnvironment (clutter etc)Body, mind and spiritWorkMoneyCheryl Richardson, Take time for your Life (1999) Step Five Con’t: Improved Work-Life Balance
What Works? 6) Developing CF resiliency through relaxation training and stress reduction techniques
Step 6 Con’t – Developing Resiliency Help for the Helper: the psychophysiology of compassion fatigue and vicarious trauma
What Works? 7) Accessing Coaching/Counselling/Clinical Supervision as needed
•Increased recognition that this is an organizational health concern (CSST report Summer 2007, Mental Health at Works CMHA and Desjardins)•The bottom line: high attrition, poor retention, soaring costs of LTD and sick leave A changing landscape, for the better
Managing workplace toxicity • Feeling wronged & bitter: A sense of helplessness, of persecution • “We become convinced that others are responsible for our well-being and that we lack the personal agency to transform our circumstances” Lipsky P93 Laura van Dernoot Lipsky (2009) Trauma Stewardship
Key Tools for Dealing with CF • Knowing your “big three”: • Your warning signs: physical, behavioural and psychological symptoms