Download
1 / 15
150 likes | 249 Views
A DIFFERENT MODEL OF CARE. Prepared by Jo Varley CNC / Team Leader Lower Mid North Coast Cluster May 2010. Lower Mid North Coast Cluster. 10,000 square kilometres. Area takes in 2 major centres Taree and Forster / Tuncurry. Mainly rural farming area.

E N D
A DIFFERENT MODEL OF CARE Prepared by Jo Varley CNC / Team Leader Lower Mid North Coast Cluster May 2010
Lower Mid North Coast Cluster 10,000 square kilometres. Area takes in 2 major centres Taree and Forster / Tuncurry. Mainly rural farming area. Small towns with limited services.
Service Network. LIAISON WITH MENTAL HEALTH OLDER PERSONS TEAM ACAT and Geriatricians AGED CARE PROVIDERS GP’S MRRH ACAT STAFF DEMENTIA SERVICE • Comprehensive Assessment Community Health TACP AGED CARE SERVICE WINGHAM REHAB UNIT t VISITS TO PRIVATE HOSPITALS
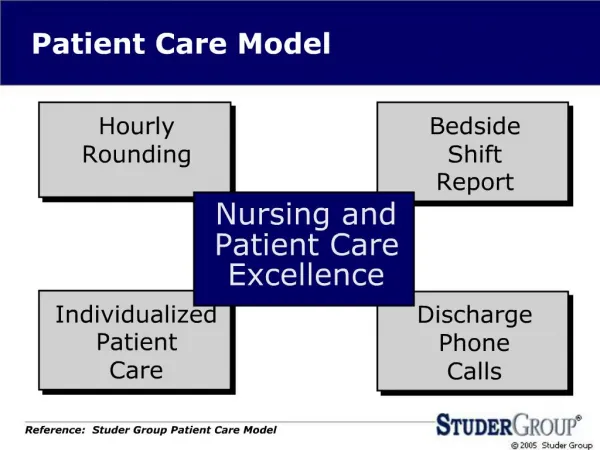
Multidisciplinary service Integrated Team that allows for sharing of staff, skills and information across the team as a whole. ACAT Nursing Geriatricians Social work Welfare Admin Aged Care Service Nursing Dementia OT’s Physiotherapy Podiatry Foot care Speech Pathology TACP Nursing OT’s Physiotherapy Domestic support
The Benefits. • Each client no matter what program they are in has the opportunity to receive interdisciplinary services. • Ability to cross refer and discuss within team leading to a more collaborative approach. • Each discipline is able to provide discipline specific services as well as a generic Aged Care focus. • Close working relationship with other community services. • Outreach clinics for small communities.
Disadvantages • The amount of travel that the service does to do assessments. • Challenges of setting up clinics in small towns. (Need a travelling road show). • The time wastage with no shows. • 6 degree’s of separation (eg I may be related to you?)
Centralised Intake Process Explain our service, eg. ACAT assessment – including Speech, OT, Physio , TACP, Dementia support, Nursing support, Social Work, Welfare Support, Podiatry, Footcare. Yes Determine with referrer if referral is appropriate for the Service. No Collect details on Intake Referral Form Give options and contact information , eg. Homecare, Kincare, Carelink, Helping Hands , and other service providers, etc. Notify the process and expected approx. wait time Offer alternatives until assessments, if available and required. NB: For complex referrals/urgent referrals a Case Discussion is held within Team Members with Team Leader and CNS ACAT. Details forwarded to Admin Intake to raise Service Request in Chime. Forward referral via Chime to appropriate service within the Team.
Central Intake Within The Team • Provides our service with: • One point of contact for all referrals • A standard referral process for all referrals. • The opportunity to discuss complex referrals prior to making the decision of who to refer to. • Coordination of referral process into the 3 arms of the service reducing risk of multiple referrals.
2008 The Big Change • In 2008 this service went from using a paper based system to CHIME. • We took the opportunity to review and redevelop our processes for management of programs, referrals and assessments. • This has resulted in flow charts that allow for staff movement between programs as needed.
Conclusion • Even though these ACAT services are in Hunter New England Area Health Service: • The needs of the communities must be taken into account. • The demographics must be considered. • Staff needs need to be considered.