Download
1 / 28
280 likes | 389 Views
Efforts to Reduce Disparities in Care for Medicare Beneficiaries. Peter B. Bach, MD, MAPP Senior Adviser, Office of the Administrator Centers for Medicare & Medicaid Services. Today. The Agency philosophy regarding health disparities Programmatic initiatives in health disparities

E N D
Efforts to Reduce Disparities in Care for Medicare Beneficiaries • Peter B. Bach, MD, MAPP • Senior Adviser, Office of the Administrator • Centers for Medicare & Medicaid Services
Today • The Agency philosophy regarding health disparities • Programmatic initiatives in health disparities • Specific health disparities initiatives • Trying to move forward • What should we do? • What can we do?
Agency Philosophy • All quality initiatives should be evaluated in light of their potential impact on the health of minority populations • Will adequate groups be included in ‘demonstrations’? • Will methodology or risk selection adversely affect minorities? • Are appropriate suites of measures being chosen to drive improvements in minority health?
Agency Philosophy cont’d • Specific quality initiatives should focus on directly addressing identified mechanisms • Should be assessed based on impact on patients, including satisfaction with care and outcomes
Mechanisms underlying disparities • Communication and comprehension barriers • Differences in access • Differences in coverage • To better define mechanisms: • Projects, interventions, demonstrations and research
Communication • National Medicare Education Program (NMEP) – 1997 BBA • Includes: • 1-800-Medicare • www.medicare.gov • Medicare & You Handbook • HORIZONS • Other
HORIZONS (Health Outreach Initiative Zeroing in On Needs) • Formed to identify strategies to reach “hard to reach” populations • Toolkits created for outreach to: • African Americans; Asian American/Pacific Islander; Hispanic American • Include: • Handbooks, print brochures, media scripts
REACH • Regional Education About Choices in Health Care • Implemented by CMS Regional Offices to increase access to Medicare information • Targets: -Low Income -Location -Language -Literacy -Culture
State Health Insurance Assistance Programs (SHIP’s) • Funded by CMS to provide counseling to Medicare beneficiaries • Specifically about issues related to Medigap and drug coverage • Counselors community based, often volunteers • Present in all 50 states + D.C. • Mandated to target underserved populations (usually defined by income) • CMS has developed training materials (English and Spanish) in counseling and cultural competency
Access • Specific concerns about lack of proper healthcare facilities locally available to minority populations • Health Care Infrastructure Improvement Program – Sec 1016 of MMA • Large loans to facilities to build-out cancer care infrastructure • Specifically targeted at geographic regions where there are large populations of Native Americans • Tremendous amount of infrastructure work focused on geographic availability of drug benefit and DME
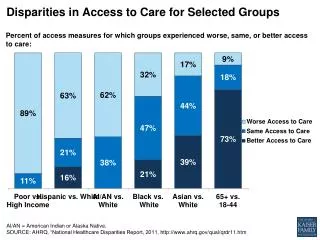
Coverage differences • Not all beneficiaries have the same coverage • Part B coverage requires co-pays and has a deductible • Minorities more likely to have Medicaid • 32% of blacks; 9% of whites • Minorities more likely to have no coverage • 20% of blacks, 14% of whites
Coverage differences • Important preventive services no longer need co-pay and do not affect deductible • Vaccines – influenza, pneumococcal, Hep B • Cancer screening – mammograms, PSA test, FOBT • Change in Part B drug reimbursement to ASP • Effect should be that physicians payments more similar when treating patients with Medicare and Medicaid than previously
Utilization and Access to Care • Health Disparities: Measuring Health Care Use and Access for Racial/Ethnic Populations • Analyzes health care access trends • Assesses validity of race/ethnicity data in the Medicare enrollment database
READII • Racial and Ethnic Adult Disparities in Immunization Initiative • CMS collaborates with CDC to improve flu and pneumococcal immunization rates • Focuses on African Americans and Hispanics • Five locations: • Chicago, IL • Bexar County (San Antonio vicinity), Texas • Milwaukee, WI • Monroe County (Rochester vicinity), NY • Selected Counties, rural MS
QIOs • Quality Improvement Organizations • Established by legislation in 1982 to improve quality of care • Present in all 50 states and U.S. territories • Undertake special efforts in health care, including specific diseasesand disparities inminority populations • QIO’s are “on the ground”, working with providers, beneficiaries, and networks
QIO Disparity Projects • 1999-2002 51 projects • 2002-2005 52 projects • Include global measures on diabetes, mammography screening, immunization, and heart failure • Two tasks in next scope • Work with providers who treat underserved to use IT more effectively (DOQ-IT) • Promote provider and practice system changes to achieve CLAS (culture and language) standards and cultural competency
Medicare Advantage Plans • Ensure that all services are accessible to all • QIO’s charged with improving care in these plans • The QAPI project requires plans also to improve cultural competence, either as manifest by reducing a clinical health disparity or by developing cultural initiatives
HBCU Grant Program • Historically Black Colleges and Universities Health Services Research Grant Program • Small applied projects awarded to: • Remove barriers and improve health • Increase efficient utilization • Improve quality • Reduce health care costs • Improve HIV and AIDS outcomes
CMS Demonstrations • Physician Group Practice Demonstration • Medicare Health Support (CCIP) • Cancer prevention and treatment
Physician Group Practice Demonstration • Awardees are 10 large physician group practices • Focuses on the quality of preventive care and ultimately on the outcomes of beneficiaries treated by the groups • Incentives for practices – better efficiency and outcomes will result in bonus payments
Medicare Health Support • Formerly the Chronic Care Improvement Program (CCIP) • Beneficiaries with specific conditions – congestive heart failure and diabetes – who reside in target regions • Regions (10) chosen for high prevalence • Chicago, DC, Georgia, Mississippi, Brooklyn/Queens • Randomized study where enrollees can receive additional care management • Objective is to enhance existing physician-patient relationships
Cancer Screening & Treatment • Cancer Prevention and Treatment Demonstration for Ethnic and Racial Minorities • Defined racial and ethnic minority groups • Sites (rural and inner city) will facilitate cancer screening, diagnosis and treatment • Charged with funding 9 sites
Screening and Treatment • Randomized designs • Invited participants: Care management organizations, health insurers, group practices, academic health centers, minority serving institutions • Two promising strategies addressed • Risk assessment assistance • Patient navigation/community health workers
Cancer Screening Demo Status • Solicitation was published in the Federal Register on 12/23/04 • Proposals were due 3/23/05 • Award is expected mid-2005 • Full-scale implementation in Fall 2005
Other Initiatives • HHS “Closing the Health Gap” campaign • Take a Loved One to the Doctor Day initiative • Broadcasts on ABC Radio Networks • Celebra La Vida Con Salud initiative • Celebrate a Healthy Life
Summary In addressing this problem, CMS: • Recognizes the magnitude of the problem • Recognizes it has a special responsibility to address the problem • Leverages all Agency resources • Seeks ideas, suggestions, and support from ALL!
FOR MORE INFORMATION 1-800-MEDICARE www.medicare.gov www.cms.hhs.gov