Download
1 / 16
160 likes | 175 Views
Bone marrow Transplant in Paediatric Haematology. Rob Wynn Consultant Paediatric Haematologist Director Paediatric BMT Programme. Understanding BMT. Two competing immune systems Donor vs Recipient Recipient wins Rejection Relapse Transplant fails Donor wins Graft versus host disease

E N D
Bone marrow Transplant in Paediatric Haematology Rob Wynn Consultant Paediatric Haematologist Director Paediatric BMT Programme
Understanding BMT • Two competing immune systems • Donor vs Recipient • Recipient wins • Rejection • Relapse • Transplant fails • Donor wins • Graft versus host disease • Remission of malignant disease • Transplant is a succes
Donor immunity recipient immunity
Supporting engraftment • Recipient ablation Donor bone marrow Myeloablative chemo- radiotherapy Time after BMT
Indications for HSCT • Malignant diseases • Chronic leukaemias • Acute leukaemias • Myelodysplasia • Myeloma • Lymphoma • Mode of Action of SCT in Malignant Disease • Graft versus Leukaemia • Intensity of Conditioning Therapy
Non malignant indications for BMT • Haematological Indications • Disorders of HSC number – aplastic anaemia, Fanconi anaemia • Red cell disorders – thalassaemia, sickle cell anaemia, Diamond Blackfan Anaemia • White cell disorders – congenital neutropenia, Schwachman Diamond • Lymphocyte disorders – immunodeficiency (SCID), Haemophagocytic syndromes • Platelet disorders – Glanzmann’s
Non malignant indications for BMT • Non haematological indications for HSCT • Enzyme deficiency • Mucopolysaccharide disorders (MPS) • Adrenoleucodystrophy • Disorders of Osteoclast function • Malignant Infantile Osteopetrosis (MIOP) • Others (experimental) • Osteogenesis imperfecta (delivering MSC) • Autoimmune disorders (delivering IS, resetting IS) • Systemic sclerosis,
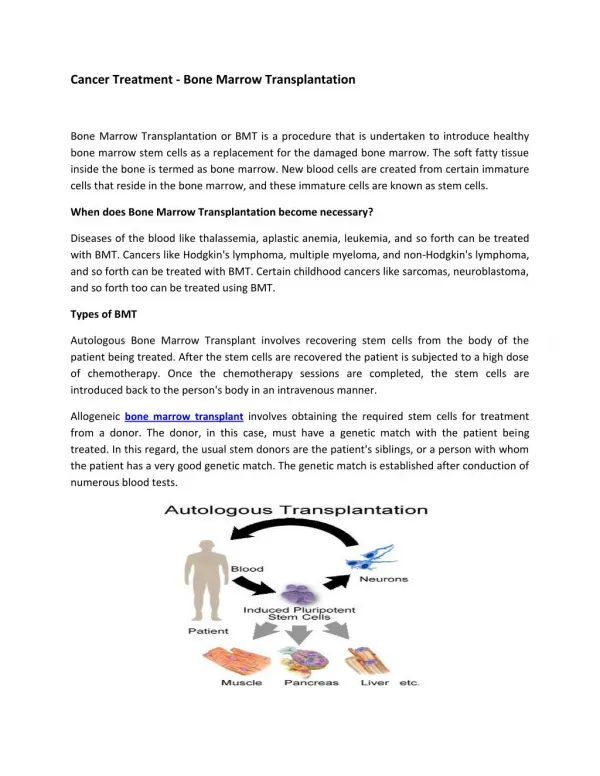
Sources of HSC • Sibling • 1:4 chance of matching where same parents • Other family members • Only where consanguinity • Haplo-identical • Parent, when desperate and need it quickly • Matched Unrelated Donor • From donor registry • Largely caucasian donors • Unrelated UCB donor pools reflect ethnic mix of population better • Autologous • Use and freeze patients own cells • +/- purging
Sources of stem cells • Bone marrrow • Perhaps 1% of marrow MNC are CD34+ • Umbilical cord blood • Perhaps 1% of CB MNC are CD34+ • Mobilised peripheral blood • Can mobilise vast quantities of CD34+ cells • G-CSF to recipient • Leukapheresis of MNC fraction
Outcomes • This is a risk balance question • Risk of disease • Natural history etc • Risk of Transplant • How well is the patient? • How well matched is the donor? • Consent will include risk of death or serious morbidity balance against risk of no transplant • Process and consent in transplant is more surgical than medical in type
Complications of transplant (1) • Complications of High Dose chemotherapy • Acute • Mucositis • Liver – VOD – weight gain, jaundice, hepatomegaly • Chronic • Infertility • Growth • Second malignancy
Complications of Transplant (2) • Infection • Early – Neutropenic • Bacterial – prophylaxis and treatment • Fungal – prophylaxis and treatment • Late • Viral • Usually fatal infection is preceded by period of asymptomatic viraemia • Screening – PCR – of blood urine stool weekly so as to intervene with antivirals in this window period • Adenovirus, CMV, EBV
Complications of Transplant (3) • Graft versus Host Disease • With HLA mismatch • Donor T cells against recipient tissue antigens • Acute • SKIN, GUT, LIVER • Grade 0 - IV • Chronic • ALL ORGANS (except brain) • Will include Graft Versus Tumour • Prophylaxis with match and ciclosporin • Treat with steroids and other immune suppression