Download
1 / 37
370 likes | 482 Views
‘The Problem in the Medicine Cabinet’ Suzy Reierson LPC SAP MAC CEAP. A Trend in Prescription Abuse. Outline - A Trend in Prescription Abuse. I. Introduction - My awareness: 2001-2010 II. What Does the Research Say? National Institute for Drug Abuse (NIDA)

E N D
‘The Problem in the Medicine Cabinet’ Suzy Reierson LPC SAP MAC CEAP A Trend in Prescription Abuse
Outline - A Trend in Prescription Abuse • I. Introduction - My awareness: 2001-2010 • II. What Does the Research Say? • National Institute for Drug Abuse (NIDA) • The Partnership for a Drug-Free America • US Department of Health and Human Services (DHHS) • III. The ‘Drugs’ Most Commonly Abused • Opiates, Depressants, Stimulants • IV. Tools, Technology, Training and Data • Substance Use Spectrum, Definitions, Strategies
I. Introduction - My Awareness of the Trend • Increase in Ads in Magazines, TV, and Internet • MDs prescribe more to avoid complaints of neglect • More medications on the market • 2002 MD at Detox Unit noted more patients in Rx detoxthan all other drugs combined • 2003 More persons on Schedule 2-4 Rx’s - EAP and Health Dept. • 2009 Dr. Oz on Oprah – 7000 new opiate addicts per day • 2009 Ongoing – New Drug Czar R. Gil Kerlikowske Nat’l problem Rx abuse • On-going: Hollywood Starsin News – Rx Overdose
NATIONAL DRUG INTELLIGENCE CENTER RELEASES • Director of National Drug Control Policy, Gil Kerlikowske said, “The 2010 National Drug Threat Assessment highlights diversion and abuse of prescription drugs as a serious and increasing problem. As part of the Obama Administration's comprehensive approach to reduce drug use and its consequences, ONDCP and Federal partner agencies have developed a plan to curb prescription drug abuse, which includes expanding prescription drug monitoring programs and educating healthcare providers and patients about the danger of abusing prescription drugs.” • A copy of the National Drug Threat Assessment 2010 can be found at NDIC’s web site at: http://cts.vresp.com/c/?HoustonEAPA/d25196b9d0/317fe6bc34/1e106ba28b
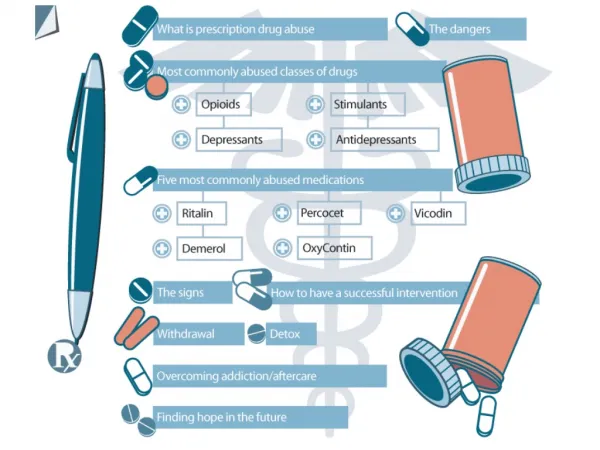
II. What Does the Research Say? • A. National Institute on Drug Abuse (NIDA) • 1. ABUSE(definition) : intentional non-medical use, not as prescribed, not responsibly & (not the DSM-IV diagnosis) • 2. Three common classes most abused: • a. Opioids – pain management • b. Central Nervous System Depressants (brain and spinal cord) – sleep, anxiety • c. Stimulants – narcolepsy, ADHD, ADD
II. What Does the Research Say? • B. The Partnership for a Drug-Free America • 1. Study Tracking Usage 2005 • a. 1/5 teens abused Rx (4.5 million) • b. 1/5 tried stimulants and tranquilizer • c. 1/10 tried cough syrup • 2. Seen as ‘safe’ to get high or self medicate • 3. Meds most used: • a. Pain – Vicoden, Oxycontin • b. Stimulants – Ritalin, Adderall • c. Tranquilizers – Xanax, Valium
II. What Does the Research Say? • C. U.S. Dept. of Health and Human Services (DHHS) • 1. 6.3 million Americans abused Rx’s in 2009 • 2. Rx abuse is on the rise due to: • Ease of obtaining (often prescribed and ‘in the medicine cabinet’) • Seen as ‘legal’ • Genetic predisposition (+ exposure when and if used in family) • For sale and profit purposes • ‘Fix-it quick’ mentality • Easy Internet access • Doctor shopping (and perhaps multiple doctors) • Start for a valid medical reason, i.e. ‘needed’
II. What Does the Research Say? • 2005 National Survey on Drug Use and Health (NSDUH) • 6.4 million persons (>12 years old) admitted to non-medical use (other than prescribed) of prescriptions during the last month • 4.7 million abused pain meds • 1.8 million abused tranquilizers • 1.1 million abused stimulants • 9% increase in young adults abusing pain relievers
II. What Does the Research Say? • DRUG ENFORCEMENT AGENCY (DEA) • Medication Diversion in Texas - 2008 • Most Abused: Hydrocodone and Pseudophedrine • Obtained by: #1 Internet,forgery, theft, doctor shopping • Also: Benzodiazepines, Oxycotin, Fentanyl, • Prometh w/codeine, Tussinex, Lortab, Buprenex, Phentermine
III. The Drugs Most Commonly Abused • Drug Abuse Warning Network (DAWN) – • ‘Prescriptions are the #1 drug of abuse’ • Hydrocodone (Vicodin, Loricet, Loritab) • Benzodiazepines (assorted) • Oxycodone (Oxycontin, Percocet, Percodan, Tylox) • Methadone • Clonazepam (Klonopin) • Propoxyphen (Darvocet N, Darvocet)
III. The Drugs Most Commonly Abused • Drug Abuse Warning Network (DAWN) – • ‘Prescriptions are the #1 drug of abuse’ • Amphetamine (Dexedrine, Ritalin, Adderall) • Lorazepam (Ativan) • Corisoprodol(Soma) • Diazepam (Valium) • Trazedone (Desyrel)
Utah Study 2008 –Adult Use of Prescription Opioid Pain Medications --- Utah, 2008 • Leftover opioid medications represent a potential danger that might be reduced with different prescribing practices and closer prescription monitoring (Box). Identifying and publicizing acceptable options for patients with leftover medications (e.g., mixing pills with an undesirable substance and throwing them in the garbage, or utilizing law enforcement drop boxes) also might increase frequency of proper disposal (9).
III. The Drugs Most Commonly Abused • Drug Enforcement Agency (DEA) • Classifications – 1970 • Schedule 1: Illegal Drugs • Schedule 2: High Potential for Abuse • Schedule 3: Some Potential for Abuse • Schedule 4: Potential for Abuse
III. The Drugs Most Commonly Abused • Who is most prone to abuse what drugs? • White • Young – stimulants • All - Opiates • Women –sedatives • All -Mix with alcohol • All-Combine Rx OTC Alcohol for suicide • All- MD, DDS, ‘gift’, black market • - DAWN trends
LINGO ….. “Going to the pharm …” • PAIN • Oxycontin Percocet VicodenUltram • hillbilly heroin percs happy pill, vikes • DEPRESSANTS • Xanax Benzos Ativan Ambien • totem poles candy, downs, sleep, tranks • STIMULANTS • Ritalin AmphetaminesAdderall • kiddy coke,, bennies, LA turnaround, ups, • Vitamin R West Coast, truck drivers • *Seen also in local private practice/treatment facility
IV. Tools, Training, Technology, Data • 4 A’s of Intervention • Aware or the trend • Alert when there are signs of possible problem • Acquirethe information needed to make informed decisions • Act to intervene via team approach and/or assessment by qualified substance abuse professional
IV. Tools, Training, Technology, Data • Continuum of Prescription Drug Use
IV. Tools, Training, Technology, Data • A. DEFINITIONS: • Physical Dependence • Active Addiction • Addiction in Remission • Pseudo-Addiction
IV. Tools, Training, Technology, Data • 1. Physical Dependence • Withdrawal symptoms occur when one stops taking or reduces the chronic drug use. • (Similar to when you stop taking Blood pressure meds, you may get hypertension.) • May exhibit drug-seeking behavior and take action to obtain the medication yet not same as addiction • Can occur whether legal or illegal drug • May occur when taking Rx as prescribed and even in presence of pain/need for Rx
IV. Tools, Training, Technology, Data • 2. Active Addiction • Current psychological dependence characterized by mental obsession • May have current physiological dependence thus withdrawal symptoms predicted and characterized by physical compulsion i.e. compulsive drug-seeking and use despite harmful consequences • Key feature is loss of control – loss of choice about their behavior • Chronic relapsing disease: neurochemical and molecular brain changes • DSM IV-TR: Dependence defined up to one month post last use • (i.e. not in remission)
IV. Tools, Training, Technology, Data • 3. Addiction in Remission • Persons in a strong recovery will forego medication even in face of trauma • Persons in remission may be at risk for triggering effect and should adhere to a protocol such as recommended by Hazelden and American Medical Association - AMA (medication monitor) as well as try less risky options • Persons in remission may also experience chronic pain and need higher doses and/or other alternative means of pain management
IV. Tools, Training, Technology, Data • 4. Pseudo-Addiction • Syndrome mimicking actual addiction • Under-treated for pain thus seeks more or self-administers not as prescribed in order to get a therapeutic effective dose of medication • Common if physician is concerned about over-prescribing for general population and more typically with person who are recovering from addiction
IV. Tools, Training, Technology, Data • Detection and Testing Issues • Test Results - Some tests do not pick up medications • Department of Transportation (DOT) – Oxycodone and Others Opiates • Professional Confusion - the ‘legal/prescribed/need’ aspects • Patient’s High Denial – “It is legal. It is prescribed. I need it”. • Disability Departments • Medical Units • Managers/HR via common Signs and Symptoms - on the job • Elder Population and Pain Issues • Recognition of Dual Diagnosis with Recovering SA Persons • Chronic Pain Issues
IV. Tools, Training, Technology, Data • Identification in Various Settings • Test to accommodate anticipated detection needs • Medical monitoring • Self-report requirement if no medical monitoring • Clear assessment protocol • Answer – ‘fit for duty’ i.e. need for treatment • Develop protocol for medical and disability settings • Create competent network & collaborate • Assist recovering persons in planning
IV. Tools, Training, Technology, Data • Assessment • Interview - develop rapport to get at details in standardized manner • Medical History – thorough and ask for Rx copies, research doctor background • Current Opioid Medication Measure (COMM) – researched and validated • Screener and Opioid Assessment for Patients with Pain (SOAPP-R) – for medical personnel
IV. Tools, Training, Technology, Data • Pain Medication Assessment • Interview Questions - See handout • Use in clinical setting as a structured interview guide • A means of data-collection • Guide for further client and team discussion • Indicators for treatment planning • Non-researched
IV. Tools, Training, Technology, Data • Current Opioid Medication Measure (COMM) * • Can be used by practitioner to document decisions • A brief patient self-assessment • To monitor pain patients • By pain/addiction & pain management experts • To identify aberrant behaviors • Examines concurrent misuse • Easy, 17 items, 10 minute, simple scoring • 500 chronic pain patients study • * To be used by individual practitioners in clinical setting
IV. Tools, Training, Technology, Data • Screener and Opioid Assessment for Patients with Pain (SOAPP-R) * • Tool to help determine how much monitoring someone may require • Addresses medical concern re: addiction, misuse, aberrant behaviors, and liability • Assist in decision-making • Overcome fear/stigma re: prescription use • *To be used by individual practitioners in clinical setting
IV. Tools, Training, Technology, Data • Use COMM when: • Long disability leave - unresolved atypical pain issue • Signs or history of abuse/addiction • Multiple meds in same family of Rx • Multiple MD’s prescribing • Pattern of behavior reflecting lack of commitment to return to work or normal daily living – malingering, defensiveness, non-compliance, evasiveness, apathy, low/no progress
IV. Tools, Training, Technology, Data • Universal Precautions – King Pharmaceuticals • Diagnose with appropriate differential – identify treatable causes of pain • Psychological assessment with risk for addiction – history of personal & family history of abuse • Informed consent – discuss and answer all questions • Treatment agreement – set boundaries to ensure expectations and patient’s responsibilities are met • Pre- and post-intervention pain assessment – level & function to assist in medication need and level decisions • Trials of medications (opiate + adjunct medication) - individualized • Reassessment – see item 5 for continuing therapy • Assessment of the 4-A’s of pain medicine: analgesia, activity, adverse effects, aberrant behavior to help direct course of care • Review of pain diagnosis and co-morbid conditions – to establish priority and changing treatment needs • Documentation – for communication and liability reduction
4 A’s: • AWARE of the trend in manner that enables us to be • ALERT when we see signs that there could be a problem so we can • ACQUIRE the information we need via investigation in order to be informed about the situation and thus be able to • ACT properly in providing that RX data to the assessor and if needed, to treatment team
TIPS for treatment: • Prescription data is best obtained through a request for all pharmacy records. We have found that relying on patient report is unreliable and often incomplete or inconsistent. • Avoid the automatic extreme reactions of ‘they do not really need this i.e. have a problem’ versus ‘they really need prescribed meds’. • Get information about all prescription history from the pharmacy and medical records from all treating MDs ASAP. • Do not rely solely on the report from the prescribing physician. • Be sure all physicians contribute their opinion on the topic. • Have each prescribing doctor write and sign a letter they are aware of what the other(s) are prescribing. • Remember than dentists can also prescribe opiates and are frequent ‘targets’ for addicted persons wishing to obtain illicit medications.
TIPS for treatment: • Have an assessment by a qualified assessor who is up to date of dealing with this sort of issues. SASSI and CAGE-AID • Utilize American Society of Addiction Medicine specialty physicians. • Be aware of your own biases re: medications. • Recognize that pain and discomfort can be addressed by many alternative means. • Be familiar with the concept of ‘medication monitors’. • Be clear on what pseudo addiction means. • Be prepared to deal with different points of view from providers. • Educate yourself about pain medicine clinics which are less than ethical and competent.
Tips for treatment: • Understand cross addiction and how that may appear in an individual. • Familiarize yourself in how to deal with persons in recovery (from Substance Dependency) who need pain treatment. • Anticipate some fears from the patient (and/or their significant others) re: ‘how will I deal with the discomfort’. • Take the time to educate the patient about addiction and cellular changes (whether the drug is legal, illicit or illegal). • Avoid underestimating the ultra high denial surrounding prescription drug dependency. • Expect here to be some issues in case managing the recovery over time – require a medication log and coordinated care.
Resources • American Society of Addiction Medicinehttp://www.asam.org/ - Site dedicated to increasing the quality of addiction treatment. Includes certification, publications, and conference info. • Centers for Disease Control and Prevention 1600 Clifton Rd. Atlanta, GA 30333, USA800-CDC-INFO (800-232-4636) TTY: (888) 232-6348, 24 Hours/Every Day - cdcinfo@cdc.gov • PainEDU – Improving Pain Management through Education www.Painedu.com • Pain Knowledge - www.PainKnowledge.org A study course