Download
1 / 66
690 likes | 1.04k Views
MALARIA: A Diagnosis We Can’t Afford to Miss!. By Tamara F. Moise D.O. Goals of Lecture. present clinical scenarios of malaria review epidemiology, life cycle, pathogenesis, clinical features, diagnosis, and treatment of malaria

E N D
MALARIA: A Diagnosis We Can’t Afford to Miss! By Tamara F. Moise D.O.
Goals of Lecture • present clinical scenarios of malaria • review epidemiology, life cycle, pathogenesis, clinical features, diagnosis, and treatment of malaria • go over the relevance of this disease as it pertains to emergency medicine
Clinical Cases • Case 1: 34 year-old Asian American male, Boston ED, 2 weeks fevers/chills, malaise, n/v • traveled to Ghana 11 months prior to ED visit for 2 weeks; + prophylaxis prior to and during his travel • visited other ED one week prior, dx’d with viral syndrome; then visited PMD (+) elevated LFT’s and thrombocytopenia
Clinical Cases • Case 2: 44 year-old Caucasian French male presented to an ICU in Marseilles, France with 3 day history of fever • 21-day trip to Gabon, Africa • (-) chemoprophylaxis
Clinical Cases • Case 3: 38-year-old Guyanese woman outpatient facility in France, 5 days jaundice • returned from a 5-day Kenya trip; in 11 days sxms started • (-) chemoprophylaxis • lived in France since infancy
Introduction • Mosquito-borne protozoan infection that primarily affects RBC’s • 5 species of Plasmodial parasite: P. falciparum, P. vivax, P. ovale, P. malariae, P. knowlesi (monkey-derived malaria) • P. falciparum deadliest • Increasing incidence due to several factors, i.e. increasing resistance of parasites to anti-malarials
Epidemiology • 300 to 500 million cases of malaria yearly; 700,000 to 2.7 million deaths • Deaths tend to occur in children in developing nations • Highest risk of transmission rural areas, end of the rainy season • Regions of greatest intensity of malaria transmission are Oceania and sub-Saharan Africa. • For example, Kenya’s rainy season can cause its population over 50-100 infectious mosquito bites per month
Epidemiology • P. falciparum most prevalent Southeast Asia, Haiti, Dominican Republic, Oceania, Amazon basin of South America, tropical Africa • P. vivax Central America, the Middle East, India • U.S. CDC reported 1528 cases of malaria in 2005, 7 fatal • Out of 775 patients in the US, 20% took malarial prophylaxis as directed per CDC
Transmission • transmitted by female Anopheles sp. mosquito; dusk until dawn • other forms of transmission • blood transfusion, congenitally acquired disease, organ transplantation, and sharing of contaminated needles • “Airport malaria” infected mosquitoes can enter a country via airplane thereby transmitting infection
Transmission Anopheles Mosquito
Transmission • anopheles is found in all US excluding Hawaii • In non-endemic areas such as the US, transmission occurs moreso via congenitally and through blood transfusion, rarely via mosquito-borne transmission
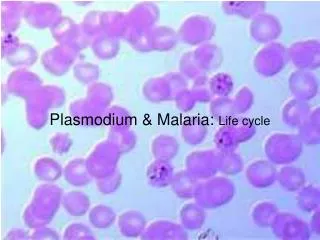
Highlights of the Life Cycle • Exoerythrocytic stage asymptomatic • Liver schizonts rupture after 6 to 16 days • P. vivax and P. ovale: • some parasites stay dormant in the hepatocytes and are known as hypnozoites; they can be reactivated and cause late relapse (months to years later)
Pathogenesis • Anemia • Hypoglycemia • Lactic acidosis • Thrombocytopenia • Microvascular dz
Pathogenesis • anemia • the parasite alters the red cell membrane, making it less deformable, resulting in hemolysis and accelerated splenic clearance, ultimately causing anemia • TNF-alpha, which is released during red cell lysis, suppresses hematopoiesis, also contributing to anemia
Pathogenesis • hypoglycemia and lactic acidosis • parasites receive their energy from anaerobic glycolysis of glucose to lactic acid, which can end up in • thrombocytopenia • Increased splenic sequestration and decreased platelet survival • microvascular pathology • falciparum forms sticky knobs on its erythrocytes’ surfaces. • this causes the RBC’s to adhere to endothelial cells of capillaries and venules sequestration of RBC’s microvascular pathology / blood flow obstruction
Pathogenesis Host Genetics • Several hemoglobinopathies protect against severe malaria, i.e. sickle cell anemia, alpha and beta thalassemias • Sickle cell anemia patients that do not live in endemic areas may not have as much protection as those living in endemic areas • Evidence has shown that sickle cell genetic alterations evolved partly due to a survival advantage against falciparum
Immunity • Semi-immune: • those who live in endemic areas develop partial immunity after repeated malarial infections • this does not prevent them from getting re-infected • Less severe disease course • Problem: • partial immunity wanes quickly after leaving an endemic area
Clinical Presentation • Erythrocytic stage • point at which patients become symptomatic • Incubation periods • P. falciparum 12-14 days • P. vivax and Ovale can be 2 months up to several years • P. malariae up to 35 days, but fever can persist for years
Clinical Presentation • Signs and symptoms are varied, but fever is present in almost all non-immune individuals • Other frequent symptoms: • headache - chills/sweats • abd pain - n/v • fatigue - cough • fevers: daily and irregular, especially in P. falciparum
Clinical Presentation • P. falciparum is unique when compared to all other malarial species because it can be fatal if untreated • whereas in P. vivax and ovale, severe disease is uncommon; it is rare in P. malariae
Clinical Presentation of P. Falciparum • High parasitemia levels; over 50% invasion of RBC’s has been reported • Highest risk of severe disease is in the following groups: • the nonimmune - children < age of 5 • pregnant women - asplenic pts • Higher degrees of parasitemia = higher mortality (nonimmune) • semi-immune pts: minimal or no clinical disease w/ high parasitemia • parasitemia level of 5% mortality rate inc
Clinical Presentation of P. Falciparum • French retrospective study 2005, studied 42 severe malaria patients b/t ’96 and ’02 , initial clinical profiles and eventual outcomes • most frequent findings: jaundice, hyperparasitemia, profound weakness; 2 patients died despite ICU intervention • conclusion: malarial patients who initially present with these findings should be considered at high risk for deterioration and death--> should be monitored in an ICU setting. *Badiaga et al. J Emerg Med 2005; 29:375-382
Complications of P. Falciparum Cerebral Malaria • altered state of consciousness and/or seizures coma or death • fatal without treatment; even with treatment, 15% of children and 20% of adults die • neurological abnormalities 10-12% of survivors • Risk factors: • extremes of age, HIV, poor nutrition, hx of splenectomy, pregnancy, genetic susceptibility
Complications of P. Falciparum • Extracerebral complications: • anemia • pulmonary edema/ARDS • renal failure • gastroenteritis
Complications of P. Falciparum • Anemia • may require transfusion • DIC may develop • Renal Failure • “Blackwater fever” : intravascular hemolysis causes large amts of Hb and malarial pigments to be present in the urine • Pulmonary edema/ARDS • Mortality rates 15% • positive pressure ventilation • Gastroenteritis • Primarily seen in children
Clinical Presentation of other Plasmodial Species P. vivax / P. ovale • symptoms identical for both • parasitemia levels 1-2% P. malariae • low grade fevers for years • low parasitemia levels (<1-2%) • mild symptoms only P. knowlesi • malarial parasite of monkeys known to cause human infection (Malaysia) • high levels of parasitemia, serious infections
Diagnosis • consider in any febrile patient who resided in or traveled to a malarial region, even if travel was brief or in transit • prompt testing when the diagnosis is suspected (falciparum) • initially missed in about 40% of US civilians who die of malaria
Diagnosis • Methods of dx: • light microscopy • fluorescent microscopy • antigen detection via HRP-2 and pLDH based serologic assays • PCR
Diagnosis Light Microscopy • Giemsa-staining of thick and/or thin blood smears conventional method of diagnosing malaria • combination is gold standard • smears allow species identification • can calculate the parasite density (prognosis) • Dependent on microscopists’ skills • 10% false negative
Diagnosis Stages of P. Vivax in thin blood smears
Diagnosis Fluorescent Microscopy • Is not as specific and sensitive as light microscopy • cannot differentiate species and special microscope is required
Diagnosis Antigen Detection Test Kits • A rapid simple dipstick test results in 10-15 minutes • useful in situations where diagnostic expertise or microscopic facilities are limited • Binax NOW first antigen testing assay FDA approved 2007 • Limitations: • cannot determine degree of parasitemia • false positives • not fully reliable for accurate species diagnosis • 2 assays currently used for testing: HRP-2 and pLDH
Diagnosis Polymerase Chain Reaction (PCR) • Has the ability to detect parasitemia at very low levels • Is helpful in species identification when microscopy is equivocal • Disadvantages are high cost, labor intensive
Treatment • supportive treatment, anti-malarial drugs • P. vivax, P. ovale, and P. malariae are mostly treated on an outpt basis • P. falciparum pts are generally admitted for observation of any complications • hospitalized until they are improving clinically and parasite count is declining • most can be treated with oral therapy severe malaria requires IV therapy/ICU
Treatment – Drug Resistance Chloroquine: • (-) resistance of P. ovale and P. malariae • new increasing resistance of P. vivax still first line for P. vivax • Chloroquine-resistant P. falciparum worldwide except for Mexico, D.R., Haiti, Central American areas west of the Panama Canal, most of the Middle East and Egypt • Chloroquine-resistance should be assumed in all pts unless clinician is absolutely certain that the pt traveled only to the areas above where resistance is not commonplace • Treating a pt who has a chloroquine-resistant strain with chloroquine puts them at increased risk of death
Treatment Tx of other Plasmodial species Tx of P.Falciparum Uncomplicated vs Severe Falciparum Malaria Tx of Falciparum Malaria in Pregnancy
Treatment of Other Plasmodial Species • Chloroquine: cure rates of 95% for sensitive strains of Vivax and Falciparum • Is still very effective for Ovale and Malariae • Primaquine is preferred treatment of P. Ovale and Vivax • Must test for G6PD enzyme deficiency before administration to avoid severe hemolysis
Treatment – Uncomplicated Falciparum Quinine: • most commonly recommended treatment for pts with chloroquine-resistant falciparum malaria • Combined w/ pyrimethamine-sulfadoxine or doxycycline • Can also combine with Clindamycin for pregnants pts or children < 8 yrs old • for semi-immune 3 day • non-immune/SE Asia pts 7 day • bitter taste, reversible tinnitus poorly tolerated
Atovaquone-Proguanil inhibits parasite electron transport for prevention and treatment well tolerated combined with Proguanil decreases resistance Mefloquine cure rates >95% in many areas causes vomiting and neurotoxicities i.e. nightmares, seizures not recommended for children <15 kg Treatment - Uncomplicated
Treatment - Uncomplicated Artemisinins • Treatment of choice for quinine-resistant P Falciparum • Should always be combined with another agent; commonly used with lumfantrine • no artemisinin-containing combination treatment has been proven to be superior to any other • Now available in US through CDC
Treatment - Uncomplicated • Many treatment guidelines consider Quinine as first-line treatment • Atovaquone-Proguanil and Artemisinin: increasingly being used due to their decreased side effects, if availability and cost are not an issue • Pts on prophylaxis should be treated with a different drug if they get infected
Treatment – Severe Malaria You have severe Falciparum malaria if: • Altered consciousness • Parasitemia of >5% • Jaundice • Oliguria • Severe normocytic anemia • Hypoglycemia • Organ failure
Treatment – Severe Malaria Malaria patients in an ICU in Cambodia
Treatment – Severe Malaria Supportive treatment is key! • Admit these pts to ICU • Aggressive fever control • If oliguria is not responding to fluids, consider dialysis • Close monitoring for hypoglycemia severe • Recommend mechanical ventilation for acidotic pts to prevent hypercapnia and rise in ICP
Treatment – Severe Malaria • Tranfuse if Hb is below 7 g/dL • Give Vit K for abnormal bleeding • Use Valium for seizures • Search for other infections and treat • be aware that pts with falciparum malaria are suseptible to gram-negative bacteremia • obtain cultures and cover for gram neg, especially for deteriorating pts
Treatment – Severe Malaria • NJ White wrote an editorial article that looked at previous studies of the treatment of severe malaria pts • One of these studies which took place in Paris showed 11% mortality among 98 severe malaria pts; another study from Vietnam show a 10-40% mortality • White commented that the relatively low mortality in Paris was likely due to aggressive renal treatment with hemodialysis and mechanical ventilation, whereas Vietnam had much less access to these modalities White NJ. Am J Respir Crit Care Med 2003;167:673