Download
1 / 37
380 likes | 641 Views
Hereditary A ngioedema. Amin Kanani, MD FRCPC Clinical Assistant Professor The University of British Columbia Division of Allergy and Clinical Immunology St . Paul’s Hospital. HAE. Hereditary Angioedema (HAE) is a rare and potentially life-threatening genetic condition.

E N D
Hereditary Angioedema Amin Kanani, MD FRCPC Clinical Assistant Professor The University of British Columbia Division of Allergy and Clinical Immunology St. Paul’s Hospital
HAE • Hereditary Angioedema (HAE) is a rare and potentially life-threatening genetic condition. • Occurs in about 1 in 10,000 to 1 in 50,000 people. • Up to 3374 of the Canadian population • Disease does not discriminate between race, ethnic groups or gender.
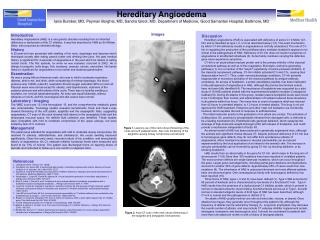
HAE Symptoms • Episodes of angioedema (swelling) in various body parts including the hands, feet, face and throat. • Swelling in the intestinal wall can cause excruciating abdominal pain, nausea and vomiting • Airway swelling is particularly dangerous and can lead to death by asphyxiation. Normal Swelling
HAE • Untreated angioedema events can last over 48 to 96 hours. • Increase frequency of attacks in puberty • Attacks varying from periodic, clustering, and variable periods of remission
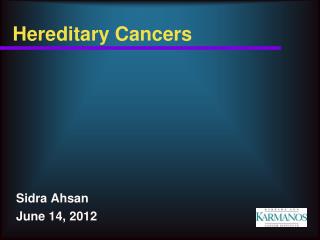
History of Hereditary Angioedema First article published by Osler describing hereditary nature With a better understand the condition, the term ‘neurotic’ has been removed from its name. Hereditary angioedema (HAE) is now the accepted named First description by Graves 1963 1882 1888 1840 Donaldson and Evans describe the absence of C1 inhibitor Quincke assigned the term angioneurotic edema
HAE • Most commonly, symptoms begin at school age • Review of 209 patients mean age at onset of the disease was 11.2 years American Journal of Medicine 2006; 119:267-274
HAE • Because the disease is rare, it is not uncommon for patients to remain undiagnosed for many years. • Unnecessary surgery has been performed on patients experiencing abdominal attacks
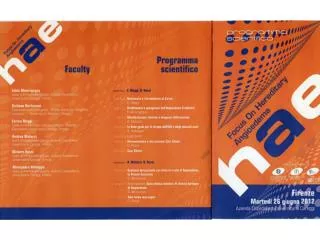
Common Triggers of HAE Attacks • Many are spontaneous Trauma Menstruation Angioedema Angioedema attack Surgical/dental procedures Pregnancy Infection Medications Estrogen ACE Inhibitor Stress
Prodromal symptoms experienced by some patients include one or more of the following: • Non-itchy red rash (Erythema marginatum) • Paresthesia (tingling, tightness, or pain) • Flu-like symptoms • Headache • Abdominal discomfort • Nausea • Fatigue • Malaise • Irritability • Mood changes • Thirst
HAE Burden of Illness • Web-based survey of 457 HAE patients found: • 100% felt disease prevented them from advancing in school • 69% felt unable to consider certain jobs • 58% affected career advancement • Impact of last HAE attack: • 51% missed ≥1 work day • 44% missed ≥1 school day • 59% missed ≥1 leisure day 1Castaldo AJ, et al. Ann Allergy Asthma Immunol. 2009;102:A92. 2Moore GP, et al. Ann Emergency Med. 1988;133:1082-1086. 3Santos C, et al. Ann Allergy Asthma Immunol.2009;102:A38.
HAE Burden of Illness • Attacks result in 20-100 days of incapacitation annually • Approximately 15,000 to 30,000 ER visits/yr • Untreated patients can lose up to 100-150 days of work per year and have morbidity rates approaching 30-40% • Unpredictability of attacks causes significant psychological burden 1Castaldo AJ, et al. Ann Allergy Asthma Immunol. 2009;102:A92. 2Moore GP, et al. Ann Emergency Med. 1988;133:1082-1086. 3Santos C, et al. Ann Allergy Asthma Immunol.2009;102:A38.
HAE is called hereditary because the genetic defect is passed on in families. • A child has a 50 percent chance of inheriting this disease if one of his or her parents has it.
HAE • Type 1 • Abnormal level of C1 inhibitor • 85% • Type 2 • Abnormal function of C1 inhibitor • 15%
Diagnostic tests • C1-INH level and/or function <50% of normal • C4 is low • Measurements should be performed twice, at an interval of at least 1 month • Testing under one year of age may not be reliable (unless genetic typing) • Genetic testing
Treatment of HAE • Education • www.haecanada.org • www.haea.org • Trigger avoidance • Carry information about condition
Canadian Hereditary Angioedema Guideline 2014 • Meeting in Toronto November 2013 • Canadian Hereditary Angioedema Network (CHAEN)/ Canadiend'angioédèmehéréditaire (RCAH) • HAE Canada • Invited most of the world experts in HAE • Reviewed all the current medical literature
Canadian Hereditary Angioedema Guideline 2014 • Treatment of Acute Attacks • Short-Term Prophylaxis • Long-Term Prophylaxis • Self-Administration • Approach to Individualized Therapy • Quality of Life • Comprehensive Care
Treatment of HAE • Acute treatment Treating an attack • Prophylactic treatment Preventing an attack
Acute Attacks • C1 INH replacement (intravenous, blood product) • Berinert 20U/kg (1000-2000 U) • Cinryze 1000 U (not approved in Canada for acute, only prophylaxis) • Icatibant (Firazyr) is a bradykinin receptor blocker. • Will be approved soon in Canada • Dose is 30 mg subcutaneously in adults • Local pain, swelling and redness at site of injection • Repeat injection 6 hours apart • Age 18 or older • Ecallantide (Kalbitor) is an inhibitor of plasma kallikrein (the enzyme that releases bradykinin) • Only approved in US not Canada
Acute Attacks • All attacks of angioedema involving the upper airway (throat) are medical emergencies and must be treated immediately. • In addition, we recommend emergency department assessment. • Laryngeal (throat) • Face, neck • Abdominal • Genital • Extremity
Acute Attacks • All patients should be trained on self-administration of HAE-specific therapies if they are suitable candidates. If patients cannot self-administer therapy, provisions should be made to ensure timely access to all appropriate therapies. • Danazol and Tranexamicacid should not be used to treat acute attacks.
Short-term Prophylaxis • To prevent an attack during a medical/dental procedure • Patient-specific trigger e.g. emotional stressor • Danazol 600 mg 5 days prior and 2-5 days after procedure • C1 inhibitor prior and second available after procedure
Long-term Prophylaxis • May be appropriate for some patients to reduce frequency, duration and severity of attacks. • Danazol • C1 inhibitor • Cinryze 1000 U 2-3 times/week • Berinert 500 U - 1000 U 2-3 times/week (not approved in Canada for prophylaxis, only acute) • Tranexamic Acid – children • It is not necessary to fail other long-term prophylaxis therapies before use of C1-inhibitor for long-term prophylaxis is considered.
Treatment of HAE Side effects may include : • virilization • weight gain • acne • hair growth • voice deepening • decreased breast size • menstrual irregularities Danazol can not be used: pregnancy, breast feeding, cancer, hepatitis, and childhood • hypertension • elevated cholesterol • altered liver enzymes • liver damage • liver neoplasms (hepatocellular adenomas or carcinomas)
Safety of C1 inhibitor products • Blood product • The specific steps of the CINRYZE and BERINERT purification process that help minimize the risk of transmitting an infectious agent include: • careful donor screening • testing for the presence of viruses • pasteurization • Nanofiltration / chromatography
Treatment of HAE • The decision to start or stop long-term prophylaxis depends on multiple factors and should be made by the patient and an HAE specialist.
Treatment of HAE • Health care providers should specifically address factors known to affect quality of life with HAE patients. Management of HAE should aim to improve patients' quality of life. • Comprehensive care should be available for all patients with HAE.
Comprehensive Care Clinic for HAE • It is recommended that HAE patients be linked with comprehensive care clinic program • bringing together clinical care, education and research • to facilitate diagnosis, therapy, management • facilitate home self infusion with C1 INH • facilitate data base registries • allow rigorous safety efficacy monitoring of emerging therapies
Emerging Therapies • Subcutaneous infusion with C1 inhibitor instead of current IV infusion • Recombinant C1-INH (Rhucin, Ruconest) • Recombinant human C1-INH produced in transgenic rabbit milk • Currently under review in the USA and Europe • BCX4161 (plasma kallikreininhibitor) is being developed as an oral prophylactic treatment for patients suffering from Hereditary Angioedema (HAE)
What Can you Do? • Don't let the disease become your identity • You can manage an illness, or it can manage you • Understand your condition and know all the options available to you • Advocate for better treatments • National program • Self infusion programs • Comprehensive care • Emerging therapies • HAE Canada
Women and HAE • Female sex hormones are known to affect the synthesis of many proteins • Estrogensensitive: the symptoms in these subjects are worsened by taking combined contraceptive medication, HRT or during pregnancy • Estrogen-independent: the use of the combined contraceptive pill or pregnancy does not exacerbate the symptoms. These individuals represent a minority of HAE patients
Women and HAE • Contraception • Progestogen pill, Depo-Provera (injection) or intra-uterine device is recommended • Pregnancy • Fertility and the rate of spontaneous abortion are the same as those found in the normal population. • Rule of thirds • 1/3 pregnancy worsens symptoms • 1/3 symptoms are improved • 1/3 remain the same • Attack rates increase during the third trimester
Women and HAE • Pregnancy • In the past treatment with tranexamic acid • Danazolis contra-indicated. • C1 INH used to treat of severe attacks • C1 INH used prophylactically if frequent attacks • The management of labour depends on how the pregnancy has progressed. • If the patient has suffered worsening of the condition then labour must be covered with C1 INH • If the disease has been less severe, there is no need for prophylaxis but C1 INH should be available • Epidural analgesia is recommended
Women and HAE • Breast feeding • Tranexamic acid, danazoland icatibant should be avoided as they are secreted in maternal milk. • Only C1 INH should be used • Menopause • In most patients (55%) the menopause does not alter the disease. • One third is worse while only 13% improve • Menopausal hormone replacement therapy should not be given because estrogencan exacerbate the condition
Women and HAE • IVF with pre-implantation genetic diagnosis • Embryo from in vitro fertilization is screened for genetic abnormalities before it is transferred into uterus