Download
1 / 99
990 likes | 1.14k Views
Diseases of the Pituitary Gland. Benjamin Glaser, M.D. Endocrinology and Metabolism Service Hadassah-Hebrew University Medical Center. Pituitary Disease. Goals of lectures: At the conclusion of the lectures and seminars (sadnaot) on the pituitary gland, the student should be able to:

E N D
Diseases of the Pituitary Gland Benjamin Glaser, M.D.Endocrinology and Metabolism Service Hadassah-Hebrew University Medical Center
Pituitary Disease • Goals of lectures: • At the conclusion of the lectures and seminars (sadnaot) on the pituitary gland, the student should be able to: • Describe the gross anatomy of the pituitary gland, and discuss the relevance of the gland's embryology and anatomy to the physiology and pathology of the pituitary. • Describe the normal control of secretion of vasopressin (ADH). • Describe the normal control of secretion of anterior pituitary hormones. • Discuss the symptoms, clinical signs, laboratory evaluation and treatment of: • Diabetes insipidus • Acromegaly • Prolactinoma • Panhypopituitarism
Posterior Clinoids Anterior Clinoids Carotids Third Ventricle Pineal Body Hypothalamus Anterior Commissure Mamillary Body Optic Chiasm Median Eminence Pituitary Human Pituitary in Sagittal Section
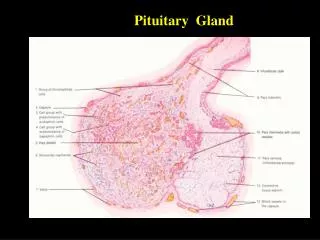
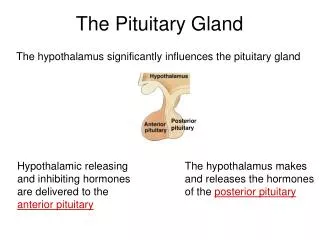
Normal Pituitary: Gross anatomy Anterior Stalk Posterior The normal gross appearance of the pituitary gland removed from the sella turcica is shown here. The larger portion, the anterior pituitary (adenohypophysis), is toward the top. The image at the left shows the superior aspect of the pituitary with the stalk coming from the hypothalamus entering it. The inferior aspect of the pituitary is shown at the right. The posterior pituitary (neurohypophysis) is the smaller portion at the bottom.
Hypothalamic releasing hormones , ADH
Third Ventricle Optic Chiasm Cavernous Sinus Infundibulum Pituitary Sphenoid sinus Normal Pituitary: Coronal MRI
Sphenoid sinus Normal Pituitary: Sagittal Section Optic Chiasm Supra Sellar fossa Infundibulum Pituitary
Human Pituitary in Coronal Section Pituitary gland Internal carotid artery III IV Cranial Nerves VI V Sphenoid Sinus
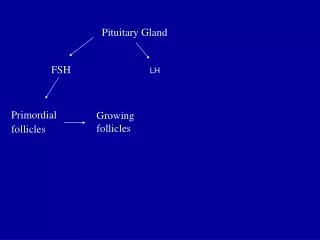
Structural disorders Trauma - stalk section Surgery Tumor Functional Hormone Producing Non-functional May affect hormone production Functional disorders Increased or decreased section of hormones LH (Leutinizing Hormone) FSH (Follicle Stimulating Hormone ACTH (Adrenocorticotrophic Hormone) TSH (Thyroid Stimulation Hormone) Growth Hormone Prolactin Diseases of the Pituitary
Pituitary Gland Hormones Thyroid Gland TSH Vasopressin (Anti-diuretic Hormone) ACTH Adrenal Gland LH FSH Oxytocin Testes/ Ovaries Prolactin GH IGF-1
Gene expression Preprohormone SP AVP NP GP AVP AVP NP GP Prohormone Production Glycosylation Proteolysis Amidation Packaging Mature Hormone Transport and Maturation Storage and release in posterior pituitary Vasopressin Biosynthesis Cell body in paraventricula or Supraoptic nucleus SP, signal peptide; AVP, arginine vasopressin; NP, neurophysin; GP, glycoprotein
Receptor-mediated effects of AVP Lee et al., Am Heart J 146:9-18, 2003
AVP regulation of water reabsorption from renal tubular cells AQP3 H2O ATP AVP AQP2 GTP(Gs) cAMP PKA H2O Endocytic Retrieval Recyclingvesicle AQP4 Thyroid hormone Glucocorticoid Dependent CollectingDuct Cell Vasa recta Collecting duct Exocytic Insertion AVP V2Receptor AQP2 Basolateral membrane Luminal membrane
Renal Concentrating Mechanism Dilute Cortex 10+ Liters/day Na H2O 300 400 Medulla H2O H2O 800 ADH Present Na H2O 1100 Na Concentrated Modified from Schrier, Renal and Electrolyte Disorders,
Renal Diluting Mechanism Dilute Cortex 10+ Liters/day Na H2O 400 Medulla H2O H2O 500 ADH Absent Na Na 600 Dilute Modified from Schrier, Renal and Electrolyte Disorders,
AVP Stimulation and Effects Pain Nausea + baroreceptors natriuretic peptides hyperosmolality hypovolemia angiotensin II + – AVP V2 Receptors V1a Receptors renal H2O reabsorption vasoconstriction Adapted from Orlandi, 2009
ADH Secretion ADH Plasma Levels ADH levels increase Markedly as soon as The plasma osmolality increases about 285 310 270 280 300 290 Plasma Osmolality
Syndrome of Inappropriate ADH Too Hot Hyperfunction Diabetes Insipidus Hypofunction Too Cold Normal Function Just right GoldilocksApproach to Endocrinology
Diabetes Insipidus ADH Deficiency
Diabetes Insipidus(ADH Deficiency) • Symptoms: • Polyuria (>2,000 cc/d) • If pituitary, usually sudden onset • Polydipsia • If pituitary, usually ice cold water • Signs • Dehydration • Hypernatremia • Normokalemia • Inappropriately dilute urine
Diabetes Insipidus • Differential Diagnosis • Osmotic diuresis (e.g. glucose) • Excessive fluid intake • Psychogenic • Central • Secondary • Nephrogenic Diabetes Insipidus • Central Diabetes Insipidus (ADH deficiency)
Genetic Chronic renal disease Polycyctic disease Pylonephritis Ureteral obstruction Advanced renal failure Electrolyte disorders Hypokalemia Hypercalcemia Drugs Alcohol Lithium Many others Miscellaneous Multiple myeloma Amyloidosis Sjoger's disease Sarcoidosis Differential Diagnosis of Nephrogenic Diabetes Insipidus (partial list):
Differential Diagnosis of Central Diabetes Insipidus • Pituitary tumor • Functioning (Prolactin, Growth Hormone etc) • Non-functioning • Craniopharyngioma • Dysgerminoma • Metastatic tumor (breast, lung) • Trauma • Surgery • Head trauma • Inflammation • Infundibulo-hypophysitis • Granulomatous disease (histiocytosis X, Sarcoid, Tuberculosis) • Genetic
Diabetes Insipidus: Clinical Evaluation • Water deprivation test: • Complete fast • Measure hourly urine and serum electrolytes, orthostatic blood pressure and weight • When plasma osmolarity ≥ 295 or urinary osmolarity is stable, then give • DDAVP 5mcg. s.c. • Interpretation: • Lack of ability to concentrate urine - DI • Good response to DDAVP - Central DI • No response to DDAVP – Nephrogenic DI
Central Diabetes InsipidusTreatment • Desmopressin (1-desamino-8-D-arginie vasopressin) • Commercial names: DDAVP, Minerin • Long-acting ADH analog • Intra-nasal -- 10-40 mcg ever 8-12 hours • Oral: 0.05 - 0.4 mg every 8-12 hours • IV/SC: 1-2 mcg every 8-12 hours • Monitor: • Electrolytes -- SIADH
Syndrome of Inappropriate ADH (SIADH) • Clinical findings: • Hyponatremia • Normokalemia • Euvolemia (mild volume expansion)
SIADH - Water and Sodium Balance • Increased ADH activity • Decreased free water clearance • Increased total body water • Hyponatremia • Increased ECF volume • Increased ECF volume • Increased GFR • Decrease proximal nephron Na+ reabsorption • Increased sodium loss • Minimizing increased ECF volume • No edema • Worsening hyponatremia
Prevalence of dysnatremias at initial presentation to a health care provider (data from 303,577 samples on 120,137 patients available for analysis) Hawkins. Clin Chim Acta 337:169-172, 2003
Symptomatic hyponatremia: neurological manifestations • headache • irritability • nausea/vomiting • mental slowing • confusion/delerium • disorientation • stupor/coma • convulsions • respiratory arrest symptomatic but less impaired; usually chronic life-threatening, usually acute
Acute hyponatremia can cause death from cerebral edema and brain herniation normal brain hyponatremic brain
Neurological symptoms are correlated with the level of hyponatremia, but with considerable individual variability across patients Arieff et al., Medicine 55:121-129, 1976
Plasma AVP levels are inappropriately elevated in most patients with SIADH 11 10 9 8 Normal Range 7 Plasma Vasopressin (pg/mL) 6 5 4 3 2 1 0 230 240 250 260 270 280 290 300 310 Plasma Osmolality (mOsm/kg) Robertson et al. Am J Med 72:339-353, 1982
Causes of SIADH Pulmonary Disorders Acute respiratory failure Infections Positive-pressure ventilation Tumors Extrathoracic Mediastinal Pulmonary CNS Disorders Acute psychosis Hemorrhage Inflammatory and demyelinating diseases Mass lesions Stroke Trauma SIADH Drugs Carbamazepine Phenothiazines Chlorpropamide Prostaglandin-synthesis Clofibrate inhibitors Cyclophosphamide SSRIs Desmopressin MAO inhibitors Nicotine Tricyclics Oxytocin Vincristine Opiates Miscellaneous HIV infection Idiopathic Pain Postoperative state Prolonged exercise Senile atrophy Severe nausea
Syndrome of Inappropriate ADH (SIADH) • Diagnosis: • Hyponatremia • Inappropriately elevated urine sodium • No volume depletion or severe volume expansion • Etiology: • Glucocorticoid deficiency • Hypothyroidism • Pulmonary lesions • CNS lesions • Drugs (Chlorpropamide) • Treatment: • Glucocorticoid/Thyroid hormone replacement (if indicated) • Water deprevation • V2 receptor antagonists (in clinical trials)
Anterior Pituitary Gland Axes Thyroid Gland TSH ACTH Adrenal Gland LH FSH Testes/ Ovaries Prolactin GH IGF-1
Distribution of Endocrine Cells in Pituitary Gonadotropin Releasing Hormone Thyrotropin Releasing Hormone Corticotropin Releasing Hormone Posterior Pituitary LH FSH 10% LH FSH 10% Growth Hormone Releasing Hormone Dopamine PRL 15% PRL 15% ACTH 20% GH 50% GH 50% Somatostatin (Somatotropin Release Inhibiting Factor) TSH 5% Stimulator of secretion Inhibitor of secretion
Pituitary Control of Thyroid/Adrenal Thyrotropin Releasing Hormone Corticotropin Releasing Hormone Thyroid Stimulating Hormone Adreno-Cortico Trophic Hormone
Loss of Pituitary Function • Functional abnormalities • Gonadotrophins -- Gonadal Insufficiency • ACTH -- Adrenal Insufficiency • Thyroid -- Hypothyroidism • GH – Growth hormone deficiency • Prolactin -- No syndrome • Anti-diuretic hormone -- Diabetes Insipidus • Structural abnormalities • Visual field disturbance • Cranial nerve dysfunction • CNS leak
Congenital Pituitary tumors Functional Non-functional Non-pituitary tumors Craniopharyngioma Metastases Trauma Surgical Head trauma Inflammation Autoimmune hypophysitis Granulomatous disease Histiocytosis X Sarcoid Tuberculosis Rathke’s pouch rupture Loss of Pituitary Function: Etiology
Anterior Pituitary Function Tests(Stimulation tests) • Thyrotrophin Releasing Hormone (TRH) • Gonadotrophin Releasing Hormone (GnRH) • Metyropone stimulation test • GH-specific tests • Clonidine, Arginine, Exercise, L-dopa • Insulin-induced hypoglycemia (ITT, IST) • Combined pituitary function test • ITT + TRH + GnRH
Hormone Replacement Therapy in Panhypopituitary Patient • Adrenal Cortex: • Dexamethasone 0.25 - 0.75 mg/d • Prednisone 5-7.5 mg/d • Hydrocortisone 15-30 mg/d • Cortosone Acetate 25-37.5 mg/d • Thyroid: • Levothyroxin 100-200 mcg/d • Maintain T4 level in upper normal range • Gonadal Steroids: • Estrogen/Progesterone or Testosterone • Desmopressin • Growth Hormone
Hypopituitarism -- Treatment • Treatment: • Hormonal Replacement • Surgical • Most tumors require surgery • Radiation • Small effect • High probability of pituitary dysfunction • Low probability of secondary tumor • May have long-term subtle neurologic effects • Medical • Steroids for hypophysitis • Specific treatment for granulomatous disease • Rarely responsive to bromocriptine or octreotide
Growth Hormone (GH) • Gene: • Chromosome 17 q 22-24 • 191 amino-acids • Protein • Species specific • Binds to 2 specific plasma proteins • Low affinity, high capacity -- significance not known • High affinity -- identical to extracellular domain of GH receptor • Absent in GH-receptor deficient states (Laron Dwarf) • Decreased in GH excess • Biologic significance • Decreased clearance? • Buffer effect? • Receptor • Highly species specific