Download
1 / 37
390 likes | 846 Views
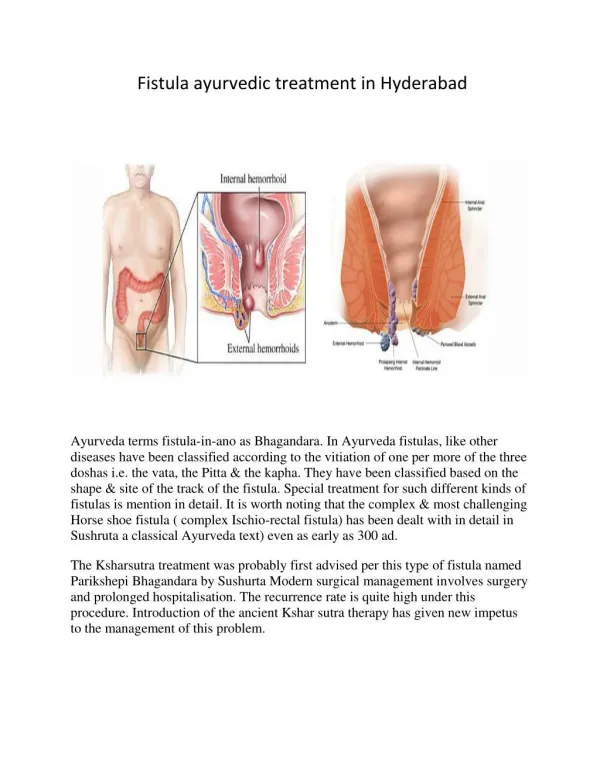
Treatment for Anal fistula. Dr. Wong Siu Wang North District Hospital Joint Hospital Surgical Grand Round Sept 2006. Classification. Parks classification Intersphincteric Trans-sphincteric Supra-sphincteric Extra-sphincteric High vs Low Simple vs Complex. BJS 1976;63:1-12. Etiology.

E N D
Treatment for Anal fistula Dr. Wong Siu Wang North District Hospital Joint Hospital Surgical Grand Round Sept 2006
Classification • Parks classification • Intersphincteric • Trans-sphincteric • Supra-sphincteric • Extra-sphincteric • High vs Low • Simple vs Complex BJS 1976;63:1-12
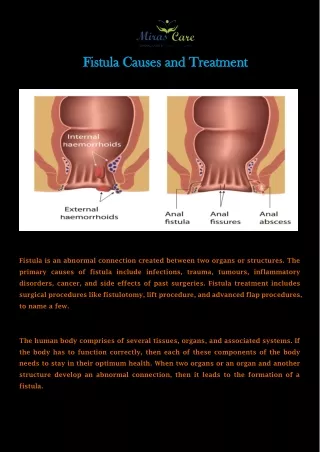
Etiology • Crytogenic • Inflammatory bowel disease • Malignancy • Tuberculosis • Pelvic sepsis
Etiology • Crytogenic • Inflammatory bowel disease • Malignancy • Tuberculosis • Pelvic sepsis
Treatment of Anal fistula • Fistulotomy • Fistulectomy • Advancement flaps • Seton (loose, cutting, chemical) • Fibrin glue • Radiofrequency
1. Fistulotomy • Standard treatment for low type fistula • Recurrence rate ~5% - 10% • Minor incontinence rate ~6% - 26% • Stage fistulotomy for high type fistula • Recurrence rate ~5% – 8% • Minor incontinence rate ~50% BJS 1995;82:895-7 BJS 1991;78:1159-61
Fistulotomy (New Modification) • Marsupialisation • Suturing the divided wound edge to the edges of the curetted fibrous track • Results in smaller wound and faster healing Colorectal Dis 2006;8:11-4 BJS 1998;85:105-107
2. Fistulectomy • Argument against fistulectomy • RCT of Fistulectomy vs Fistulotomy • Greater tissue loss leads to delayed healing • Similar recurrence rates BJS 1985;55:23-7
Fistulectomy • Argument supporting fistulectomy • Complete specimen for histology • Reduces risk of missing secondary tracks • Similar incontinence rate • Modification: • Core out technique • Fistulectome
Fistulectome The fistulectome: a new device for treatment of complex anal fistulas by “Core-Out” fistulectomy. Dis Colon Rectum 2003;46:1566-71
Fistulectome • Device for core out fistulectomy • Remove 2mm thickness of fistula tract • Limited experience and results Dis Colon Rectum 2003;46:1566-71
3. Endorectal advancement flap • Treatment for high type fistula • Close the internal opening with flap • Mucosal flap for proximal fistula, anocutaneoeus flap for distal fistula • Contra-indication: acute sepsis, large internal opening, heavily scarred rectum
Endorectal advancement flap • Results in high type fistula • Heterogenous, depend on length of FU • Recurrence rate ~20% - 60% • Incontinence rate ~18.7% Int J Colorectal Dis 1994;9:153-7 Int J Colorectal Dis 2006 Mar 15
4. Seton • Loose Seton • Cutting Seton • Chemical Seton
i. Loose Seton • Drainage of sepsis before definitive treatment (eg. Staged fistulotomy) • Primary treatment for complex fistula
Loose Seton • Procedure in St Mark’s Hospital • Tracks and extensions outside sphincter laid open • passage of Seton thro’ primary track across the external sphincter and tied loosely • Outpatient review, remove Seton at 2-3 months if wound healed
Loose Seton • Result for treatment of complex fistula • Success rate 44% - 78% • Minor incontinence rate 17% - 36% Int J Colorectal Dis 1989;4:247-50 BJS 1990;77:898-901
ii. Cutting Seton • Analog to staged fistulotomy • Cutting the fistula track with tightening of Seton • Balance between healing speed vs continence • Material: silk, braided polyester, rubber band, Penrose drain
Cutting Seton • Results are heterogenous • Average cutting time ~14-20 wks • Recurrence rate ~5% (0-29%) • Minor incontinence rate ~50% • New Modification • Snug Seton
Snug Seton • 1mm elastic Seton • Silicon nerve vessel retractor • Slow fistulotomy • T M Hammond et al • 29 patients idiopathic fistula (~38% high type) • Median cutting time 24 wks • No recurrence • Minor incontinence rate ~25% Colorectal Dis 2006;8:328-37
iii. Chemical Seton • Kshara sutra, derived from plants (Ayurveda) • Antibacterial, anti-inflammatory properties, alkaline • Weekly insertion • Slowly cut though the tissues
Chemical Seton • RCT comparing chemical Seton with fistulotomy in low type fistula • More painful with chemical Seton but no difference in healing time, complications or functional outcome Tech Coloproctol 2001;5:137-41
5. Fibrin glue • Fibrinogen solution +/- antibiotics • Promote healing thro’ fibroblast migration and activation, formation of collagen meshwork • Before injection • Curettage all granulation tissue and debris • Contraindication: acute sepsis
Fibrin glue • Results variable • For complex fistula • Successful rate ~50% • Septic complication 3% Dis Colon Rectum 2005;48:2167-72 • For simple fistula • RCT fibrin glue vs conventional treatment for anal fistula • 42 patients • No advantage for fibrin glue over fistulotomy in simple fistula Dis Colon Rectum 2002;45:1608-15
6. Radiofrequency • Radiofrequency scalpel • Fistulotomy/ fistulectomy • High frequency 4MHz radiowave • Mode: cutting, coagulation, fulgurate, bipolar
Radiofrequency • Principle • Transmit radio wave to tissue • Cause tissue damage by intracellular heating • Low cutting temperature 60 – 900C (vs 750 – 9000C in diathermy) • More precise cutting, less surrounding tissue damage, less tissue edema and pain
Radiofrequency • Two small scale randomized trial • Diathermy fistulotomy vs Radiofrequency fistulotomy/ fistulectomy in low type fistula • Less post-operative pain • Earlier return to work • Shorter wound healing time • No difference in complication & recurrence Eur Rev Med Pharmacol Sci 2004;8:111-6 Rom J Gastroenterol. 2003;12:287-91
Treatment of Anal fistula SUMMARY
Simple fistula • Standard treatment • Fistulotomy +/- Marsupialisation • Fistulectomy • Other treatments • Radiofrequency fistulotomy/ fistulectomy (emerging evidence) • Fibrin glue (lower healing rate, no advantage) • Seton (prolong healing)
Complex fistula • Initial treatment • Loose Seton (low incontinence rate) • Other treatment • Advancement flaps (variable result) • Fibrin glue (variable result) • Cutting Seton (high incontinence rate) • Snug Seton (need more evidence) • Stage fistulotomy (high incontinence rate)
Treatment for Anal fistula ~ End of presentation ~
Treatment of anal fistula Question and Answer
Definition (variable) • High type • Involving the anorectal ring • Internal opening above dentate line • Complex type • High type • Multiple side branches • Chronic inflammatory disease (Chron’s) • Previous operation/ irridation
Incontinence scoring system • Cleveland Clinic scoring system • Wexner Continence grading scale • Material: solid, liquid, gas • Frequency: rare to always
Fistulotomy and immediate reconstruction • Reconstruct the divided musculature and primary wound closure • For low type fistula • Study from Parkash et al • 120 patients • 98% low type fistula • 88% wound healed by 2 weeks • Recurrence rate 4% ANZJ Surg 1985;55:23-7
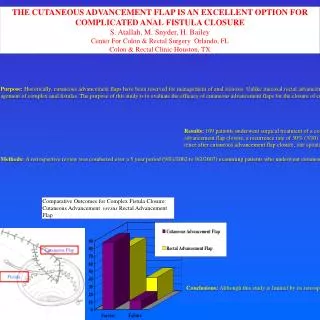
Fistulotomy and immediate reconstruction • For complex fistula • Prospective study by Perez F et al • 35 patients with complex anal fistula • 85.7% high trans-sphincteric, 11.4% supra-sphincteric, 2.9% extra-sphincteric • 31.4% incontinent patients reported improvement in continence scores • 12.5% continent patients reported minor alternations of continence (Wexner Continence Scale <4) • Recurrence rate 5.7% J Am Coll Surg 2005;200:897-903