Download
1 / 43
440 likes | 458 Views
Larry Robbins. M. D. lrobb98@aol.com WWW.ChicagoHeadacheClinic.com. Refractory Chronic Migraine (RCM). Disclosure. Speaker for Merck( Belsomra ) PI for Allergan CGRP Study PI for Teva Post-traumatic CGRP study

E N D
Larry Robbins. M. D. lrobb98@aol.com WWW.ChicagoHeadacheClinic.com Refractory Chronic Migraine (RCM)
Disclosure • Speaker for Merck(Belsomra) • PI for Allergan CGRP Study • PI for Teva Post-traumatic CGRP study OFF-LABEL: Most of this talk presents off-label material; there are nomedications indicated for “refractory headache” EVIDENCE BASED: Most of the meds discussed have had no RCTs; there are very few well done RCTs for refractory approaches.
Questions • 1.T/F: Medication Overuse Headache is easy to identify but difficult to treat • 2.T/F: Migraine surgery is a reasonable option for refractory patients • 3.T/F: Comorbidities often determine where we go with therapy • 4.T/F: Botox is our 3rd best preventive, and the FDA 155units is the only dose that is effective. • 5.T/F: Resilience has a strong genetic component
Refractory Chronic Migraine • Chronic Migraine (CM) = 2% of population • RCM Definition: • Non-pharmacological treatments are not effective • Multiple Preventives = no help. Patient failed at least 3(of the 5) classes of preventives • Medication Overuse Headache (MOH) = If present, MOH should first be addressed. MOH should not be the primary problem.
RCM: ??’s & Challenges • Diagnosis/Definition: Work in progress • Role of disability is debatable • ?? Biomarkers for CM: (scans or labs) • Severity: Mild / Moderate / Severe: does this influence treatment/our approach
??’s & Challenges, cont. • RCM may change over time, even revert to episodic • At different ages treatments vary • MOH: Definition and role; how important is MOH • New Daily Persistent Headache (NDPH): Different than transformed migraine, often more refractory
Pathophysiology • Central Sensitization • Genetics • Structural Changes (white matter)
Pathophysiology, cont. • MOH: How does it change the brain? • Psychiatric comorbidities: do the brain’s structural changes that accompany longstanding psychiatric conditions contribute to RCM?
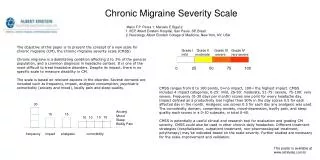
RCM Scale • A number of factors go into the scale: • Years, Associated Medical and Psych Comorbidities, Resistance to Preventive and Abortive, etc. • Mild – Moderate – Severe RCM • Is this scale helpful? (clinically, possibly for research)
MOH:How Much Does It Contribute? • Definitionis inaccurate: you cannot define MOH simply based on a set # of days of analgesics/triptans per month • Need evidence that the analgesic actually causes increased headache. • Epidemiologic studies of MOH may not be valid
Addressing MOH • Not easy!! • Many strategies; rarely is inpatient necessary • We say: “Don’t take this, don’t take that.” Patient says: “Fine, but I need to function, what do I take?” What the patient CAN TAKE is often not addressed.
Outside of Meds • Minimize Meds “It takes a village”: Get other villagers involved! • Psychotherapy • Physical Therapy • Massage • Acupuncture
Outside of Meds, cont. • Exercise • Pilates / Yoga • Mindful Meditation: • Meditation Apps: Calm, Headspace, Insight Timer • Biofeedback
Key Non-Medication Concepts • Catastrophizing: dial it down • Catastrophizing “ by proxy”: spouses or parents • Resilience factors: genetics(serotonin transporter gene), psych comorbidities, social, upbringing…. Can we improve resilience?...(Maybe)
Non-Medical Concepts, cont. • Acceptance: we can improve acceptance…“Lack of acceptance by proxy” in spouses/parents • Coping: Promote active coping Passive coping predicts disability Functioning: Improving functioning is a goal, but not easy to achieve
Caretakers & Headache Doctors • Caretakers: Difficult position, they need support Psychotherapy may help For other family/friends: also difficult for them • Headache doctors(and neurologists): High rate of burnout (50% or more) Many strategies to minimize burnout Staff burnout should also be addressed/minimized
Outpatient Therapy Options • No good algorithm: everyone is different • The “Art of Headache Medicine”: (available in a separate article) • Some of the factors that influence our treatment decisions: • Headache history, patient age, medication history(past, present),patient preference and input, sensitivity to meds, med overuse, medical comorbidities, psych. Comorbidities(particularly bipolar and personality disorders), sleep, GI, weight, fatigue, associated neck/back/arthritis pain, social aspects, job requirements, addiction history, finances(can they afford Botox, etc.), family history of med. Response, Nocebo and Placebo by Proxy, etc. • AND, of course your intuitive Gestalt: what will work, what will not…
Selected Outpatient Options Some of the options include: • Botox -Polypharmacy - Cannabis - SPG Blocks • ONB/TPIs - Frequent Triptans - Opioids - Stimulants - MAOIs • Miscellaneous:methylergonovine/ergotamine memantine - muscle relaxants - TMS - VNS ketamine - neurostimulation - SPG stimulator “Migraine surgery(anterior)” – “Trigger Point Deactivation(posterior)” - CGRPs- Oxytocin
Botox • Safe, effective for 60%long-term: although probably less than 50% continue, for various reasons • FDA protocol(155 units) OR: • “Chase the pain” • Lower doses may be effective
Botox, cont. • Off Label: • Cluster(less effective than for migraine) • Temporomandibular Disorders (TMD) : often effective for clenching • Adolescents • Mechanism of Action: • Possibly via CGRP: dampening the neuroimmune response
Polypharmacy Some patients need 2 or 3 preventives (& Botox) To determine “rational polypharmacy”: We need input from the various factors discussed previously(headache and med history, med and psych comorbidities, insomnia, GI, weight, fatigue, etc.)
Medical Cannabis • May help pain, anxiety, or insomnia • Many patients vape(do not smoke) 2X per day • The % of THC, CBD, and other oils is individualized; and some use one mixture in the morning, and another at night. It takes awhile to achieve the best mixture for any one patient. • Cannabis may help minimize(or eliminate) the use of benzos/opioids • We need more studies; anecdotal results are encouraging.
Cannabis,continued • Long-term adverse effects still not that well known • “Probably safe” but: memory in certain patients may be affected. Dependence may occur; may also decrease motivation • Try and avoid in younger patients(below age 24)
SPG Blocks (for frontal pain) • Since 1914 • Newer devices (Tian, Allevio, SphenoCath), OR: a TB syringe with an atomizer(much less expensive) • 1 or 2 times per week for 2 to 4 weeks; then some continue long-term • No SPG protocol is well established • Helps temporarily(days to weeks); Home use is possible(with atomizer device)
Occipital Blocks and Trigger Point Injections (TPI) • Primarily for posterior pain • Adding in corticosteroids helps some patients; avoid cortisone in areas that have exposed skin, in case resorption occurs • These may stop a cycle, help temporarily; may be combined with SPG blocks, or in same sitting as Botox
Frequent Triptans • Previous Study: 118 patients: Averaged 4 years on frequent triptans • MOH a major concern • Looks “relatively” safe • Triptans: 25 year safety track record
FrequentTriptans, cont. • Minimize dose, try ½ tablet; crucial to limit • Naratriptan / frovatriptan: “Kinder and Gentler” • Can always re-try preventives or Botox at any point • Avoid with major cardiac risk factors
Opioids • Effective for a small subset of RCM patients; some may obtain relief, without overuse, for decades • Many concerns: legal, regulatory, producing hyperalgesia, addiction, misuse/overuse • Opioid prescribers are often denigrated by other physicians or pharmacists
Opioids,cont. • “Rules for Success with Opioids” • 1. Avoid moderate to severe personality disorder (particularly: borderline, antisocial, paranoid); avoidant and dependent PD are usually ok. • 2. Non-addictive personality, no previous addiction(with some exceptions) • 3. Try and avoid younger than age 28
Opioids,cont. • 4. To start long-acting opioids: they had to do well on short-acting opioids, without overuse • 5. No(or minimal) tolerance to analgesic effects: This is the KEY! MOST DO BECOME TOLERANT to the analgesic effects • 6. Stick to low doses: this is crucial for a # of reasons
Stimulants • May help comorbidities: ADHD, depression, fatigue • Help with weight control • Stimulants = long record of safety(80 years of use) • While analgesic effect is usually mild, for some stimulants are surprisingly effective for headache, particularly for those who respond to caffeine
Stimulants,cont. • Methylphenidate: (Ritalin, Ritalin LA) vs. mixed salts: (Adderall, Adderall XR); Vyvanse is a “pro-drug” of amphetamine • Use low doses • Be careful with younger patients; there is very little abuse after age 23.
Monoamine Oxidase Inhibitors (MAOIs) • For refractory depression and headache In the 1980’s: commonly used(prior to SSRIs) • Diet less restrictive than before • Side effects: usually well tolerated: less SE than tricyclics – Weight gain, insomnia are common
MAOIs,cont. • Phenelzine (Nardil): the most effective Low doses: 1 or 2 at night: Can go up to 4 or 5 per day Night use minimizes food interactions • Emsam Patch (selegiline): safer, but less effective Fewer restrictions at lower doses(6mg patch); 9mg=usual dose; one metabolite of Emsam is amphetamine.
Miscellaneous • Methylergonovine (Methergine): 0.2mg • 3 to 6 per day (TID dosing) • Expensive, need fibrosis testing(if used for over 4 months), take breaks; supply goes off and on • Ergots: Ergomar(SL), 2mg: available again; minimize the dose; use for short periods of time • Memantine: occasionally may help; NMDA antagonist • well tolerated, safe • May help Mild Cognitive Impairment(MCI)
Miscellaneous,cont. • Muscle relaxants: also may help neck pain, insomnia • Non-addicting muscle relaxants: cyclobenzaprine, lioresal, methocarbamol, metaxalone, tizanidine, orphenadrine • TMS: (eNeura Spring TMS): Occipital home unit may help; may be used preventively, probably safelong-term • Probably more effective for migraine with aura; long-term efficacy is unknown. About $170 per month
Misc., cont. • Ketamine: IV or Nasal Spray(preferred) • For refractory depression and headache; probably more effective for the depression. DEA/Regulatory issues are concerns • Nasal spray = well tolerated, may be more effective in long runThe IV form =more side effects, expensive • Nasal spray: low doses, usually in office, 1 to 2X weekly; home use is possible. • Long-term side effects unknown • If effective: take breaks every 3 months
Misc., cont. • Neurostimulation: techniques and equipment have improved; occasionally helpful • Long-term satisfaction is not truly known • Lead migration, failures, re-surgeries are common • Autonomic Technologies, Inc. Sphenopalatine ganglion (“ATI SPG”) implant: promising: tested primarily for cluster; no leads/wires/batteries; successful in Europe;
Misc,cont. • Migraine Surgery(anterior, by plastic surgeons): generally poor outcomes; not recommended. However, trigger point deactivation(posterior), in experienced hands, may help. Few surgeons have the experience necessary. Need more studies. • CGRP antagonists(monoclonal antibodies): very promising: Injection every 1 to 3 months (preventive) there are 4 companies finishing Phase 3………Long-term safety is unknown. May be available by mid-end of 2018. The CGRP abortive tablets(small molecule) are being tested. • Oxytocin: fairly safe, use 20 U 2 to 3X per day; may help moods; need studies….
Questions • 1.T/F: Medication Overuse Headache is easy to identify but difficult to treat(F) • 2.T/F: Migraine surgery is a reasonable option for refractory patients(F) • 3.T/F: Comorbidities often determine where we go with therapy(T) • 4.T/F: Botox is our 3rd best preventive, and the FDA 155units is the only dose that is effective(F) • 5.T/F: Resilience has a strong genetic component(T)
References • Marteletti et al. Refractory chronic migraine: a consensus statement…J Headache Pain, 2014;15:47. • Robbins,L. Difficult to treat chronic migraine: outpatient approaches Scientific American Neurology Oct. 2016 (published online). • Goadsby PJ, et. al. Refractory migraine and chronic migraine: pathophysiological mechanisms. Headache 2008; 48: 799-804. • Robbins,L. Refractory chronic migraine: long-term follow-up using a refractory rating scale. J Headache Pain 2012; 13: 225-229. • Sahai-Srivastava et al. Multidisciplinary team therapy approaches to CDH Headache 2017; 57(9): 1482-1491.
References,continued • Lai TH, Wang SJ. Update of inpatient therapy for refractory CDH. Curr. Pain and Headache Reports 2010; 20(1): 5. • Cady RK et al. Long-term efficacy of repetitive sphenopalatine blockade….Headache 2015;55:529-42 • Miller, S. et al. Predictors of response to occipital nerve stimulation in refractory chronic headache Cephalalgia 2017 Jan1,Epub. • Robbins, L. A practice guide for continuous opioid therapy for refractory daily headache headache Headache 2010; 50:1614.
References, continued • Robbins, L. Difficult to treat chronic migraine: outpatient medication approaches. Practical Pain Mngt 2014; 14(8) 32-43. • Mathew PG, Robbins L. Cranial neuralgia vs entrapment neuropathy decompression… Headache 2015: 55; 706-710