Download
1 / 41
470 likes | 897 Views
Melatonin and Sleep. Garrick Wang, M.D., Ph.D. Stanford Sleep Disorders Clinic Stanford Dept. of Psychiatry . What is melatonin?. Hormone that is naturally produced by the pineal gland Conveys information to various parts of the body Chemical structure identified in 1958

E N D
Melatonin and Sleep Garrick Wang, M.D., Ph.D. Stanford Sleep Disorders Clinic Stanford Dept. of Psychiatry
What is melatonin? • Hormone that is naturally produced by the pineal gland • Conveys information to various parts of the body • Chemical structure identified in 1958 • Expressed rhythmically throughout the day
Regulation of Melatonin • In the US, the FDA considers melatonin a “dietary supplement” • No need for a prescription • No regulation of dosing and preparations may have additives that affect bioavailibility, side effects, drug interactions • Not detected in food
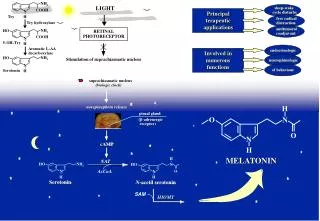
Making Melatonin • Generated from amino acid tryptophan and serotonin • Is made predominantly at night in the pineal gland • Freely diffuses into bloodstream and crosses blood-brain barrier
Making Melatonin • Generated from amino acid tryptophan and serotonin • Is made predominantly at night in the pineal gland • Freely diffuses into bloodstream and crosses blood-brain barrier
Where Melatonin Binds • Works by binding 3 receptors • MT1 = Found in the SCN of hypothalamus, pituitary gland, cardiac blood vessels • MT2 = Retina and hippocampus • MT3 = Kidney, brain, other organs
SCN: Our internal clock • Suprachiasmatic Nucleus (SCN) is the site of internal biological clock • Many intrinsic properties cycle: cortisol, body temperature • Melatonin binding MT1 inhibits neuron activity
How Melatonin Works • Melatonin levels cycle • Low levels during daylight, rise during nighttime • Peak levels between 11PM and 3AM • Levels continue to cycle in constant darkness • Can slowly adjust to environmental changes
Melatonin Activity • Light acts indirectly, likely through retina, to inhibit melatonin synthesis and release • MT1 and MT2 receptors desensitize: activity decreases after exposure to excessively high levels of melatonin
Melatonin Secretion • Melatonin secretion starts at 3-4 months of age when nighttime sleeping consolidates • Peak levels at 1-3 years of age • Slightly lower levels through early adulthood • Marked decline in levels afterwards • Peak levels for 70 year olds is ¼ of levels for young adults
Melatonin Levels • Exogenous melatonin of 1-10mg raise levels 3-60x normal nighttime levels • Doses as low as 0.1 to 0.3 mg caused dose-related decreases in sleep latency and self-reported sleepiness and fatigue • Blood levels did not go above nighttime levels
Melatonin Activity • Metabolized by the liver • Propranolol, caffeine, and alcohol can interfere with melatonin activity • Vitamin B6 needed for synthesis. Estrogen, OCPs, hydralazine, lasix may affect levels • Levels can also be affected by preparation. Those in oil-based preparation lead to higher blood levels
Adverse Effects • Excess melatonin can lead to daytime sleepiness, impaired mental and physical performance, hypothermia, and high levels of prolactin • Menstrual irregularities, galactorrhea, impotence, decreased libido
Melatonin and Sleep Promotion • Analysis of 17 separate studies looking at people who slept normally or insomnia from a number of causes (e.g. age, jet lag, Alzheimer’s, schizophrenia) • Melatonin can decrease sleep latency (time between laying down and onset of sleep) • 4 minute decrease on average • Works in afternoon and evening as well
Melatonin and Sleep Promotion • Melatonin also increased sleep efficiency. • Sleep efficiency = amount of time asleep as percentage of total time in bed • Increase in total sleep duration of 12 minutes
Significance? • Hard to determine significance due to wide variations of studies • Doses ranging from 0.1 to 80 mg • Wide variety of subjects: sleep latency normal for most elderly, sleep efficiency not very affected for jet lag
Melatonin and Insomnia • Looking more closely at those with insomnia secondary to neurologic or psychiatric disease, as well as jet lag or shiftwork, melatonin did not help • Implies effectiveness for primary insomnia
Other Studies • Doses as low as 0.3 mg can decrease sleep latency, increase sleep duration and sleep efficiency without affecting body temperature. • Melatonin at early evening to help for prolonging elevated nocturnal melatonin levels (useful for shift workers and jet lag)
Melatonin and Insomnia • One study showed improved sleep efficiency in adults >50 yo vs. controls • No changes seen in total sleep time or sleep architecture • No changes seen in patients without insomnia • 0.3 mg effective and resulted in peak concentrations similar to young adult peaks
Melatonin and Insomnia • One study showed improved sleep efficiency in adults >50 yo vs. controls • No changes seen in total sleep time or sleep architecture • No changes seen in patients without insomnia • 0.3 mg effective and resulted in peak concentrations similar to young adult peaks
Melatonin and Insomnia • One study showed improved sleep efficiency in adults >50 yo vs. controls • No changes seen in total sleep time or sleep architecture • No changes seen in patients without insomnia • 0.3 mg effective and resulted in peak concentrations similar to young adult peaks
Melatonin and Sleep Architecture • No consistent changes in sleep architecture • Unlike hypnotic medications used to promote sleep, subjects reported they could fight off sleep if they wanted to • In addition, no reports of cognitive impairment in the morning
Ramelteon (Rozerem) • Synthetic melatonin agonist that acts at MT1 and MT2 receptors • Approved for treatment of insomnia • No potential for abuse
Melatonin and Phase Shifting • At night, advances the clock. In early AM, delays clock • If given at 5PM, can advance nighttime melatonin secretion • 0.5 mg can also shift body temperature rhythms • Can also entrain rhythms in blind individuals who did not have endogenous rhythms
Melatonin and jet lag • Especially useful for Eastbound travel • Shown effective if taken at bedtime of destination when crossing >5 time zones. • Improved total sleep time • Less effective westbound • Adverse effects include dizziness, headache, decreased appetite, daytime sleepiness
Other uses of melatonin • Although thought to have antioxidant properties and thus useful for atherosclereosis, cancer, and Alzheimer’s, no controlled clinical data supports this. • In vitro studies needed concentrations 1000 to 100,000 times normal levels • At such levels, may impair sleep and circadian rhythms by desensitization
Other uses of melatonin • No improvement in cognitive impairment in Alzheimer’s patients • No evidence as helpful for anti-aging • Small studies suggest melatonin may reduce blood pressure
Adverse Effects • Daytime sleepiness, Hypothermia • Desensitzation of melatonin receptors if doses too high • Possible adverse events in those with seizure disorders • Possible interaction with those taking coumadin/warfarin
Conclusions • For problems of sleep efficiency (such as age-related insomnia), melatonin starting at 0.3 mg. If no effect after a week, can double dosage. • If initial response but stops being effective after a few weeks, recommend “drug holiday”
Conclusions • For traveling > 5 time zones, take melatonin at bedtime of destination up to 4 days after arrival • May also consider for travel < 5 time zones if jet lag would be serious interference • 0.3 to 0.5 mg recommended starting dose
Conclusions • Effectiveness may depend on cause of sleep problems • Must be aware of different forms of packaging and dosing • Inform physicians if interested in a trial of melatonin