Download
1 / 40
400 likes | 421 Views
THE BASICS OF RISK MANAGEMENT. Housekeeping. STRUCTURE FOR THE DAY. Risk Management recap Risk Management under the microscope Tools and Techniques Patient Safety Case Study. Risk Management recap. Risk is …. The management of UNCERTAINTY to increase the probability

E N D
STRUCTURE FOR THE DAY • Risk Management recap • Risk Management under the microscope • Tools and Techniques • Patient Safety Case Study
Risk is …. • The management of UNCERTAINTY to increase the probability • of success and reduce the probability of failure. • Risk is inherent to any activity, has the potential to affect your success, and can be both negative and positive. • With risk comes opportunities for growth and development. • It can be shaped but not totally eliminated!
What is Risk Management in NHS Scotland • Risk management is the systematic identification, assessment and reduction of risks to patients, staff and the organisation (NHS HIS) • Risk management proactively reduces identified risk to an acceptable level by creating a culture founded on assessment and prevention rather than reaction and remedy. (NHS HIS) • The aim of risk management is to create a culture in which NES staff and stakeholders are aware of risk and its potential impact, and in which they are aware of their responsibilities in relation to the management of risk, thereby promoting an open and responsive approach to risk management which actively involves all elements of NES. • (NHS Education for Scotland)
Benefits of Risk Management • Supports strategic and business planning • Promotes continuous improvement and identification of new opportunities • Encourages innovation and creativity • Engenders a proactive outlook • Ensures robust contingency planning • Improves our ability to meet objectives and achieve opportunities • Reduces shocks and unwelcome surprises • Advocates transparency • Furthers compliance with governance agenda • Stimulates regular review and monitoring of business processes • Enforces ownership • Provides for effective use and prioritisation of resources • Reassures staff, stakeholders and governing bodies • Enhances communications internally and with external stakeholders • More informed decision-making.
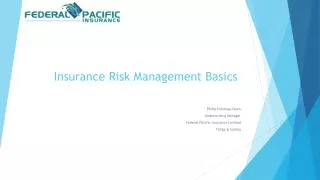
Identifying and Managing a Risk Monitor and review Identify the risk Plan / implement additional actions Evaluate the risk Manage the Risk Risk response (ownership and priority)
How to identify a Risk - some questions to ask • Risk Management relates to the identification of uncertainties and what actions could be taken to mitigate against them, or even encourage them. • * Has this event happened before in our organisation (or a team) or in another similar organisation? Could it happen again? • * What are the key dependencies / core processes / routine operations of our organisation (or a team)? Are there any possible things that could affect their continuity? • * What are our main objectives? What might prevent them from being achieved? • * Are there any new activities / developments / products / improvements that could impact existing functionality or bring in new risks for us (or a team)? What can be done in mitigation? • * What opportunities are there that we could benefit from? • * Does the event relate to our Accountability/Governance requirements; our Financial position; our Operations / Service Delivery; our Reputation or Credibility; Health & Safety?
Sources of Risks • Risks to the project / function / activity’s existence • - strategic direction / policy change; funding / staff withdrawal • Risks from within the project / function / activity • - overspending; over-run; poor quality end-product • External Risks (more difficult to predict) • - customer / stakeholder pressures; socio-political pressures; environmental pressures
Identifying and Managing a Risk Monitor and review Identify the risk Plan / implement additional actions Evaluate the risk Manage the Risk Risk response (ownership and priority)
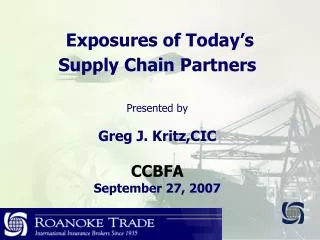
(yes) TERMINATE? (no) (yes) TRANSFER? (no) (yes) TREAT? (no) TOLERATE Evaluate the Risk - Risk Decision Path removes risk eradicated, however inaction may lead to other risks reduces likelihood of loss PROACTIVE risk subcontracted risk occurrence insured against controls in place to reduce likelihood of risk occurring reduces impact REACTIVE actions in place to deal with risk when it occurs
Identifying and Managing a Risk Monitor and review Identify the risk Plan / implement additional actions Evaluate the risk Manage the Risk Risk response (ownership and priority)
Prioritising Risks • In NHS Scotland Risk is measured in terms of its impact and likelihood: • Impact - a reflection of the pain or loss or discomfort that may be caused by an event • Likelihood - an indication of how often we can expect a particular event to occur • In NHS Scotland, risk is scored on a 5 x 5 matrix and ranges from negligible to catastrophic • Risk is summarised into Low, Medium (Housekeeping or Contingency) and Primary risks.
Managing a Risk - jargon • Corporate Governance • The system by which companies are directed and controlled • Event • The occurrence of a particular set of circumstances • Mitigation • The act of making a consequence less severe • Issues v Risks? • Risks are things that might happen, issues are things that are actually happening • Controls v Actions? • Controls are mitigation measures already in place, actions are new controls that we are currently working on.
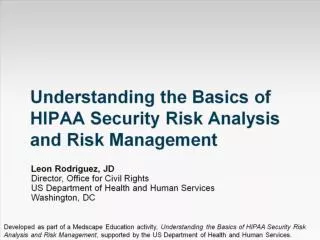
The Cumulative Act EffectThe SWISS CHEESE of Risk Management James Reason 1990
Inadequate communication Reasons for latent failure
Significant Event Analysis (SEA) • Carried out in individual cases in which anyone in the team thinks there has been a significant occurrence (not necessarily involving an undesirable outcome for the patient) are analysed in a systematic and detailed way to ascertain what can be learnt about the overall quality of care and to indicate changes that might lead to future improvements
Root Cause Analysis (RCA) • A structured approach to identifying the factors that resulted in the nature, the magnitude, the location, and the timing of the harmful outcomes (consequences) of one or more past events in order to identify what behaviours, actions, inactions, or conditions need to be changed to prevent recurrence of similar harmful outcomes and to identify the lessons to be learned to promote the achievement of better consequences.
Problem Solving - Some tools and techniques • Bono’s Six Thinking Hats • Brainstorming • PEST(LE) • SWOT • Five Why’s / So What • Ishikawa Fishbone • Barrier Analysis • Significant Event Analysis • Root Cause Analysis
Barrier Analysis • Technique used in Root Cause Analysis or Significant Event Analysis, and can be used reactively to solve problems or proactively to evaluate existing barriers. • The term “barrier” is used to mean any barrier, defence or control that is in place to increase the safety of a system. • Four types of barrier – Physical; Natural; Human Actions; Administrative • Identify the process to be reviewed • Identify all control measures in place • Ensure you have Physical and Natural barriers (failsafe) • Consider additional control measures that would be useful • Consider the cost:benefit of additional measures • Assign ownership and action new additional measures • Repeat regularly (Proactive Barrier Analysis Dineen 2002)
Inadvertent Harm • This is a case study prepared by the National Patient Safety Agency in England and is based on a real incident. • In 1968, vincristine was first administered intrathecally (ie into the spine) in error to a young patient with acute lymphocytic leukaemia. She died 3 days later. • Intrathecal administration of vincristine is a rare event but catastrophic for the patient, family and clinical team involved. Over 40 years, 58 cases of intrathecal vincristine errors are known to have occurred across the world.
Timeline - characters Jazmin Munroe Consultant Charlotte Green Pharmacist Tech Mr Shah Pharmacist Jane Hughes Patient Duncan Campbell New Specialist Registrar Liam Short Staff Nurse Helen Roberts Relief Sister Abe Kamole Staff Nurse Fiona Livingstone Specialist Registrar Joe Robinson Relief Junior Doctor Ann Lynch Ward Sister
Inadvertent harm – timeline variations • Before the day • Patient and Consultant agree to IV and IT treatment on same day • On the day • Pharmacist issues Vincristine (IV) and Methotrexate (IT) • Ward Sisters in charge unable to handover at shift change • Patient arrives late • Ward SpR unexpectedly leaves Ward • Patient taken to dedicated bay and plugs into her walkman • Staff Nurse called away to emergency • Locum SpR and SHO left alone to administer chemotherapy drugs.
Inadvertent Harm • Thinking back to your pre course reading: • What prevention barriers were in place? • Did the barrier work? • If it failed, why? • How did the barrier affect the consequence of the event? • What could you do to try to prevent an incident of healthcare associated harm occurring in the future? • What lessons could be learned from such an incident?
No Blame • In NHS, when a serious incident occurs, in order to fully learn from the event, a policy of no blame is taken (you don’t usually come to work planning to deliberately harm someone or do a bad job!) • But what could the pharmacy staff in particular have done differently? • Vincristine (IV) and Methotrexate (IT) should not have been issued on same day, Pharmacist raises concern but is over-ridden; • Pharmacist Technician knows she should not dispense the Methotrexate (IT) to someone who is not on the register, but is over-ridden; • Pharmacist Technician does not confirm that the Vincristine (IV) has been administered before dispensing the Methotrexate (IT); • Pharmacist Technician does not confirm that the Methotrexate (IT) will be administered immediately to the patient and not stored on the ward.
Inadvertent Harm – an afterthought • Route delivery errors account for approximately 5% of medication errors. (Bates DW, Boyle DL, et al “Relationship between medication errors and adverse drug events.” J Gen Intern Med 1995;10:199–205.) • Such incidents attract serious incident enquiries and proposals have been made involving the physical redesign of delivery systems such that it is impossible to deliver drugs by the wrong route. • To date, an international agreement on such standardisation is yet to be reached.
Summary - We are all risk managers • Everyone in the organisation is involved in the management of risk • Risk is a proactive tool in supporting and informing decision-making • Any time is a good time to review the risks in your work area and plan mitigations to prevent them / cope when they occur • If you are commencing a new project or large piece of work, your planning would be aided by considering the risks and introducing controls to mitigate against them happening or take steps to reduce their impact if they are not preventable.
Today we have covered • Risk Management recap • Risk Management under the microscope • Tools and Techniques • Case Study
Thank you for participating Any questions?