Download
1 / 66
850 likes | 1.44k Views
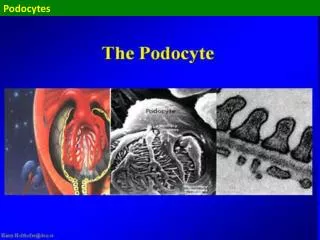
Podocytes. Podocytes . the filtration barrier = an amazing structure filtering something like 200-500 l plasma per day and producing something like 200 l of primary urine

E N D
Podocytes the filtration barrier = an amazing structure filtering something like 200-500 l plasma per day and producing something like 200 l of primary urine the podocyte which is really standing or sitting on top of the capillaries is one of the key players there in the final regulation of the passage of the proteins or actually preventing the leakage of the proteins
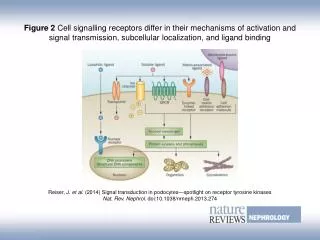
Podocytes there is a number of molecules located in the slit diaphragm domain transmembrane or intracellular these molecules adjust the shape of the podocyte foot processes
Podocytes Nephrin - neph-1, neph-2, filtrin, hemoglobulin group of molecules, an immunoglobulin family of cell adhesion proteins They are clustering together with podocin for the functionality of the slit diaphragm The nephrin molecules extend from neighbouring podocytes and foot processes and induce the interaction between the different podocyte foot processes Nephrin really forms the framework of the slit diaphragm
Podocytes The nephrin damage determines lack of normal foot processes and the filtration slit organisation Specific administration or generation of specific nephrin antibodies lead to proteinuria In diabetes and diabetic nephropathy there are found circulating anti-nephrin antibodies many months before the actual attack to the kidney
Podocytes there are quite a number of podocyte diseases = podocytopathies in the podocytopathies the orderly structure of the podocytes and the foot processes interlinked by the slit diaphragms is lost (effacement of the podocytes
Glomerulopathies - patterns of glomerular injury the glomerulus interconnected between the efferent and afferent arterioles the general patterns of glomerular injury reflect the picture that we can see in the biopsy of a patient with either nephrotic or nephritic syndrome translates to the clinical symptoms with which the patient presents
Glomerulopathies scanning electron micrograph the arterials and the capillary network
Glomerulopathies the structure the efferent and afferent arteriole the both lined with continuous endothelium fenestrae in the glomerular capillaries in which the endothelium ends up smooth muscle cells surround the efferent and afferent arterioles have kind of retracted to the mesangium area no longer covere the capillaries
Glomerulopathies the basement membrane between the fenestrated endothelium and the epithelium on the outside the capillary network is interconnected between the efferent and afferent arterioles the constriction governs the blood flow profusion pessure in the capillary network allows solutes to pass over the capillary wall under normal conditions - without proteins or cells
Glomerulopathies a closer look at the scheme the capillary wall functions as a sieve the profusion pressure and flow of the capillaries the passage and filtration of small molecules over this sieve major determinants of their filtration the molecular and physical properties of the molecules that are filtered over the structure of the capillary wall
Glomerulopathies The capillary wall can be seen as a gel it is also used in the lab in chromotography to separate molecules based on their size and charge
Glomerulopathies the sieve can be injured the patterns of injury
Glomerulopathies The capillary wall is a porous network negatively charged due to the heparin sulphate proteoglycans multiple mucopolysaccharides on the surfaces of cells The filtration of larger molecules - retarded The filtration of negatively charged molecules - retarded very important for the filtration of albumin
Glomerulopathies Filtration is determined not only by the size and charge of the molecules but also by their molecular configuration for example: a globular molecule (the same molecular weight as a dextrin) is retarded because it cannot unfold in contrast to the dextrin molecules
Glomerulopathies The negative charge it is not only important for the physiology of filtration it also has a down side charge of the capillary wall can easily bind, attract, and expose positively charged molecules that bind to the negative charges here; for example, histone DNA-complexes in nucleosomes that are circulating in our circulation all the time can easily bind due to the positive charge of the histone proteins to this negative charged wall and then be exposed to the circulating auto-antibodies directed to DNA
Glomerulopathies The same is true for positively charged streptococcal and other bacterial cell walls circulate after an infection bind to the capillary wallexposer to antibodies form immune complexes binding to the capillary wall leads to an increased capacity to bind antibodies
Glomerulopathies Electron micrograph the capillary wall the fenestrated endothelium the basement membrane made up of the various components produced by the epithelial cells also by the endothelial cells
Glomerulopathies On the epithelial cells the arborised cell with its processes interconnected through the slit membranes the process of 1 cell adheres to the process of its neighbouring cell there is a constant contact between 2 different cells over this interconnection important for filtration characteritics important for the functioning of the epithelial cell
Glomerulopathies Normal glomerulus the capillary tuft fills up the Bowman's space almost adheres to Bowman's capsule, but it is still detached from it Bowman's capsule is thin, it is not thickened the tubules are close together the peritubular capillaries - inconspicuous the mesangial and endothelial cells –almost inconspicuous
Glomerulopathies Severely injured glomeruli -for example a severe post-streptococcal glomerulonephritis a lot of inflammation in the capillaries that have collapsed a lot of extracapillary proliferation infiltration with neutrophils in the Bowman's space and crescent a lot of fibrin in the extracapillary space in the capillary lumina
Glomerulopathies This is a bit extraordinary for a post-streptococcal glomerulonephritis usually is not extracapillary but you can get this kind of injury as well (severe form) pathogenic mechanisms endothelial injury activation of complement and other proteasescoagulation and inflammation
Glomerulopathies Proteases cascades complement in those 2 glomeruli activation and deposition of complement C3
Glomerulopathies The different pathways along which complement and other reactants can lead to glomerular injury (I)The start an antibody complement activation endothelial injury detachment from the basement membrane denudation and exposure of the extracellular matrix complement activation endothelial injury due to cytotoxic agents from bacteria thrombotic events complement activation
Glomerulopathies Considering glomerular antibody deposition as 1 mechanisms by which complement can become bound and activated (II) Antibodies by themselves directed to certain surface molecules such as epithelial cells FC-receptor bindinginjury to glomerular cells (more important than complement binding) Complement binding direct toxic injury to the glomerular cells Complement binding binding and splitting off several components lead to chemotactic factors recruit neutrophil,’ platelets and macrophages to the glomerular capillaries cytotoxicity
Glomerulopathies Glomerular cells react with their own response to injury (III) glomerular cells, invading macrophages production of chemokines recruition T cells come in and play their role in the inflammatory reaction products of these cells: oxygen radicals and proteases glomerular cells injury proteinuria, hematuria, low of the GFR
Glomerulopathies There are several plasma serine proteases and cascades involved in inflammatory injury in the glomerulus
Glomerulopathies The way to understand what happens in the biopsy how to read and translate the biopsy to the clinical expression Is that the glomerular injury is largely determined by the localisation of injury either by immune complexes or by other stimuli
Glomerulopathies For example immune complexes localise under the endothelium or along the basement membrane the binding and activation of complement recruition the leucocytes endothelial pattern of injury
Glomerulopathies Endothelial pattern of injury Etiology post-infectious glomerulonephritis anti-GBM nephritis proliferative forms of lupus Clinically drop in GFR , hematuria, sometimes with proteinuria Biopsy inflammation and exodation
Glomerulopathies Another pattern of injury - epithelial pattern injury at the external of the basement membrane under the epithelium complement activation or a direct effect of substances that are toxic to the epithelial cell epithelial injury
Glomerulopathies Epithelial pattern in membranous nephropathy in membranoproliferative glomerulonephritis in lupus type V Clinically associated with heavy proteinuria Biopsy there is no inflammation
Glomerulopathies Epithelial pattern - there is no inflammation because the injury that happens here complement activation activated complement leaking through the capillary wall complement components cannot go back into the capillary lumen they cannot function as chemotactic agents there will be no recruit of inflammatory cells they will be lost into the urinary space they can be found and measured in the urine
Glomerulopathies Glomerular injury due to deposition of immunoreactants or other reactants in the mesangial area IgA nephropathy membranoproliferative glomerulonephritis lupus type II
Glomerulopathies Examples to illustrate a patient with post-streptococcal glomerulonephritis infiltrating neutophils intravascular coagulation with fibrin some neutrophils escaping into the extracapillary space
Glomerulopathies Examples to illustrate the same patient with post-streptococcal glomerulonephritis this is associated with massive deposition of C3
Glomerulopathies Examples to illustrate the same patient with post-streptococcal glomerulonephritis electron microscopy the basement membrane on the outer side the podocyte on the inside very swollen endothelial cells the lost of endothelial fenestrae this is in reaction to an inflammatory reaction to the immune reactants = the dark deposits containing IgG and especially complement at the inner side of the basement membrane
Glomerulopathies Examples to illustrate the same patient with post-streptococcal glomerulonephritis electron microscopy a neutrophil eating up these deposits on the inside of the capillary wall there is also epithelial injury
Glomerulopathies Endothelial pattern of injury - rapid decline of GFR endothelial injury due to antibodies anti-GBN nephritis Good Pasture's syndrome systemic vasculitis idiopathic cresentic GN(probably a limited form of ANCA-associated vasculitis) endothelial injury not due to antibodies but due to endothelial injury because of other causes bacterial cytotoxins malignant hypertension immune complex deposition in lupus nephritis and membranoproliferative
Glomerulopathies Examples to illustrate a patient with anti-GBN disease - an endothelial pattern of injury extracapillary proliferation Broken Bowman's capsule infiltration into the periglomerular area
Glomerulopathies Examples to illustrate a patient with anti-GBN disease - an endothelial pattern of injury electron microscopy typical wrinkling of the injured basement membrane do not see real immune deposits because they are located all along the basement membrane
Glomerulopathies Examples to illustrate another patient - an endothelial pattern of injury a systemic vasculitis - Wegener's granulomatosis segmental spared part of the glomerulus a segmentally involved part of it with fibrin exodation, inflammation, and extracapillary proliferation
Glomerulopathies Examples to illustrate another patient - an endothelial pattern of injury an acute phase malignant hypertension arterial injury and thrombosis in the same pattern in the glomerulus leading to acute renal failure
Glomerulopathies Endothelial pattern of injury - rapid decline of GFR Some of these diseases - quickly heal Sometimes - find some sequele A lot of these diseases - will continue to go on