Download
1 / 36
360 likes | 748 Views
Briefing: ICD-10-CM (International Classification of Diseases – 10 th Revision – Clinical Modifications) A Piece of Cake. Date: 23 March 2010 Time: 1400–1450 . Pre-Quiz. Quiz – jot down your answers 1. ICD- 10 -CM is

E N D
Briefing: ICD-10-CM(International Classification of Diseases – 10th Revision – Clinical Modifications)A Piece of Cake Date: 23 March 2010 Time: 1400–1450
Pre-Quiz Quiz – jot down your answers • 1. ICD-10-CM is • a. ICD-9-CM where they replaced the three digit categories with three digit alpha-numeric categories to have more space • b. Pretty much volumes 1 and 2 of ICD-9-CM (volume 3 is now ICD-10-PCS) • c. Mapped to ICD-9-CM with about 95% of the codes being a one-to-one mapping • d. All of the above
Pre-Quiz • 2. When you think “Personal History of” you think – • a. V10 – Personal History of malignant neoplasm, through V15 Other Personal History Presenting Hazard to Health • b. V86 Estrogen Receptor Status • c. V87 Other specified personal exposures and history presenting hazards to health • d. V88 Acquired absence of other organs and tissue • e. Both a and c even though they are not in the same place – this just makes coding more challenging!
Pre-Quiz • 3. The coding guidelines for ICD-10-CM (e.g., assign all the digits available) are • a. Are pretty much the same as for ICD-9-CM. • b. Are pretty much the same as for ICD-8-A. • c. Are pretty much the same as for ICD-7. • d. Are pretty much the same as for ICD-6. • e. All of the above.
Pre-Quiz • 4. The ICD-9-CM codes are being “frozen” (will not change, no additions/deletions) in 2012 because • a. There is so much automation and all those programs need to have all the code numbers for the various conditions changed, tested, fixed, tested… • b. To give coders an entire year to goof off claiming they were studying VERY hard to understand the ICD-10-CM. • c. Because the cost of gasoline had gone up to $5/gallon and those of us driving up from Washington to Baltimore for the Coordination and Maintenance Meetings wanted a break for an entire year. • d. Because we knew Washington DC was going to get 30+ inches of snow in one week and we wanted all the coders to know how to spell “frozen” before December 2009 and February 2010.
Pre-Quiz • 5. The General Equivalency Mappings (GEMs) don’t have a one-for-one mapping because • a. Some few medical concepts have changed so the ICD-10-CM reflects the thought process of the current medical understanding. • b. ICD-10-CM has expanded some concepts so it may have five codes while ICD-9-CM only has one code. • c. If there was a one-for-one mapping to ICD-9-CM from ICD-10-CM, and a one-for-one mapping to 10 from 9, why bother with ICD-10? • d. All of the above. • e. None of the above.
Pre-Quiz • 6. I plan to get ready for the new codes: • a. On 1 Oct 2013 and not a second before. • b. When I take the Oct 2013 AHIMA CCS-P quiz I will borrow a book and hope for the best. • c. I’d be willing to attend teleclasses for a few weeks prior so long as they let me do it from work • d. What – you silly goose, who actually believes the MHS will be ready on 1 Oct 2013, they can’t even get the new codes out until Jan/Feb/Mar on a normal year – I’m sticking with the MHS and plan never to have to learn the new codes • e. Other:
Objectives Know that ICD-10-CM transition will be easy for coders Understand the General Equivalency Mappings Know the coding guidelines for ICD-10-CM
ICD-10-CM • Why • How – Direct Care • Issue: CAPER (Comprehensive Ambulatory/Professional Encounter Record) diagnosis field is only 7 characters • Issue: SIDR (Standard Inpatient Data Record) diagnosis field is only 8 characters • Issue: AHLTA (Armed Forces Healthcare Longitudinal Tracking Application) • Issue: CCE (Coding Compliance Editor) • Issue: All the other direct and purchased care MHS (Military Healthcare System) systems/programs using ICD codes • Training Proposal Development • Coders • Providers • Data Analysts
Difference Between ICD-10-CM,ICD-10-PCS and ICD-9-CM • International Classification of Diseases – 9th Revision – Clinical Modifications (ICD-9-CM) • Developed in USA in 1970s based on the World Health Organization’s ICD-9 • Based on ICD-8, and ICD-8a • Clinical Modifications (CM) is the United States’ version • Added to WHO ICD-9: • External Causes of Injury • Factors Influencing Health • Volume 3, Institutional Procedure Coding
ICD-10-CM • ICD-10-Clinical Modifications is for use in the United States • Other countries use modifications specific to their country, such as ICD-10-CA for Canada and ICD-10-AM for Australia • ONLY: • Diagnoses, • Factors Influencing Health, and • External Causes of Injury • Does not include procedures as did ICD-9-CM • No third volume • See ICD-10-Procedure Classification System • Currently used for cause of death reporting in the United States
ICD-10-CM • Available for download from: • http://www.cdc.gov/nchs/icd/icd10cm.htm#10update • At the bottom of the page • A bit easier and less expensive than going to Ingenix and buying it on disc for $119.00 • Would recommend buying one book every other year until 2013 as they are much easier to work with • The downloads are nice for a quick word search
ICD-10-CM Is Better Due To • Addition of information relevant to ambulatory and managed care encounters • Expanded injury codes • Creation of combination diagnosis/symptom codes to reduce the number of codes needed to fully describe a condition • Addition of a sixth character for some codes • Incorporation of common 4th and 5th digit subclassifications • Laterality; and • Greater specificity in code assignment for many codes. • The new structure will allow further expansion than was possible with ICD-9-CM.
ICD-10-CM • “Piece of Cake” for anyone who can code using ICD-9-CM • Same basic guidelines • Same basic layout/organization • Same basic index • Same basic tabular • Some codes are more detailed • Some codes indicate initial or subsequent encounter • Format – alpha + 2 numerics + decimal point + numeric+3 alphanumerics • H66.9 Otitis media, unspecified • Otitis media NOS • Acute otitis media NOS • Chronic otitis media NOS • H66.90 Otitis media, unspecified, unspecified ear • H66.91 Otitis media, unspecified. right ear • H66.92 Otitis media, unspecified, left ear • H66.93 Otitis media, unspecified, bilateral
Review of Existing Code Formats • ICD-9-CM diagnoses (look for the decimal point) • 3-5 numeric characters with decimal point after the 3rd • External cause of injury Exxx.x • Factors influencing health Vxx.xx • ICD-9-CM procedure (look for the decimal point) • Numeric xx.xx • CPT – 5 numeric, or 4 numeric with terminal F or T (no decimal point) • HCPCS – alpha with 4 numeric (no decimal point) – does not currently use F or T
ICD-9-CM ICD-10-CM Chapt Title Category Chapter Title Category er Range Range I Infectious and parasitic diseases 001-139 I Certain infectious and parasitic diseases A00-B99 II Neoplasms 140-239 II Neoplasms C00-D48 III Endocrine, nutritional and metabolic 240-279 III Diseases of the blood and blood-forming D50-D89 diseases and immunity disorders organs and certain disorders involving the immune mechanism IV Diseases of blood and blood-forming 280-289 IV Endocrine, nutritional and metabolic E00-E90 organs diseases V Mental disorders 290-319 V Mental and behavioral disorders F00-F99 VI Diseases of the nervous system and 320-389 VI Diseases of the nervous system G00-G99 sense organs VII Diseases of the circulatory system 390-459 VII Diseases of the eye and adnexa H00-H59 VIII Diseases of the respiratory system 460-519 VIII Diseases of the ear and mastoid process H60-H95 IX Diseases of the digestive system 520-579 IX Diseases of the circulatory system I00-I99 X Diseases of the genitourinary 580-629 X Diseases of the respiratory system J00-J99 system XI Complications of pregnancy, 630-676 XI Diseases of the digestive system K00-K99 childbirth and the puerperium XII Diseases of the skin and 680-709 XII Diseases of the skin and subcutaneous L00-L99 subcutaneous tissue tissue ICD-9-CM Comparison to ICD-10-CM
The Tabulars • ICD-9-CM • 001 Cholera • 001.0 Due to Vibrio cholerae • 001.1 Due to Vibrio cholerae el tor • 001.9 Cholera, unspecified • 002 Typhoid and paratyphoid fevers • ICD-10-CM • A00 Cholera • A00.0 Cholera due to Vibrio cholerae 01, biovar cholerae (classical cholera) • A00.1 Cholera due to Vibrio cholerae 01, biovar eltor (cholera eltor) • A00.9 Cholera, unspecified • A01 Typhoid and paratyphoid fevers
The Tabular – Example J00 (Currently 460) Excludes1 = NOT CODED HERE (both conditions cannot occur at same time Excludes2 = Not included in this diagnosis, if it is there, code them both
ICD-9-CM vs ICD-10-CM Tabular • ICD-9-CM 8. Diseases of the Respiratory System (460-591) Acute Respiratory Infections (460-466) 460 Acute nasopharyngitis [common cold] • ICD-10-CM Chapter X – Diseases of the Respiratory System (J00-J99) Acute Upper Respiratory Infections (J00-J06) J00 Acute nasopharyngitis [common cold]
ICD-10-CM • Morbidity classification • Includes potentially fatal conditions • Treatable • For use in • Hospitals; acute short-term, long-term • Provider office • Other outpatient settings
Benefit to the MHS • Ability to • Collect more detailed information • Compare morbidity data to mortality data • Compare to international data • Collect some laboratory results (e.g., blood alcohol levels and ABO blood types)
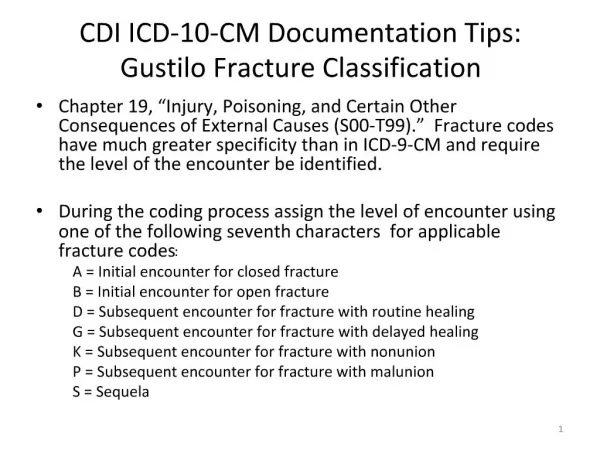
Benefit to the MHS • Ability to collect concepts such as • “Do Not Resuscitate” • Initial versus subsequent encounters • Right, left, bilateral • First, second, third trimester • Identification of fetus in multiple gestations • Classifications of fractures • Dominate versus non-dominate side • Burns separated based on heat or chemical • Cesarean delivery without medical indication
Benefit to the MHS • Better data on which to base decisions • Easier to pull records with criteria needed for a specific study • Expandable, more space for new conditions • More detailed external causes of injury • e.g., Y93.5B Cellular telephone usage in work-related activity
Example of Expanded Code Set • F10.2 Alcohol dependence • Excludes1: alcohol abuse (F10.1-) • alcohol use, unspecified (F10.9-) • Excludes2: toxic effect of alcohol (T51.0-) • F10.20 Alcohol dependence, uncomplicated • F10.21 Alcohol dependence, in remission • F10.22 Alcohol dependence with intoxication • Acute drunkenness (in alcoholism) • Excludes1: alcohol dependence with withdrawal (F10.23-) • F10.220 Alcohol dependence with intoxication, uncomplicated • F10.221 Alcohol dependence with intoxication delirium • F10.229 Alcohol dependence with intoxication, unspecified • F10.23 Alcohol dependence with withdrawal • Excludes1: Alcohol dependence with intoxication (F10.22-) • F10.230 Alcohol dependence with withdrawal, uncomplicated • F10.231 Alcohol dependence with withdrawal delirium • F10.232 Alcohol dependence with withdrawal with perceptual disturbance • F10.239 Alcohol dependence with withdrawal, unspecified • F10.24 Alcohol dependence with alcohol-induced mood disorder • F10.25 Alcohol dependence with alcohol-induced psychotic disorder • F10.250 Alcohol dependence with alcohol-induced psychotic disorder with delusions • F10.251 Alcohol dependence with alcohol-induced psychotic disorder with hallucinations • F10.259 Alcohol dependence with alcohol-induced psychotic disorder, unspecified • F10.26 Alcohol dependence with alcohol-induced persisting amnestic disorder • F10.27 Alcohol dependence with alcohol-induced persisting dementia • F10.28 Alcohol dependence with other alcohol-induced disorders • F10.280 Alcohol dependence with alcohol-induced anxiety disorder • F10.281 Alcohol dependence with alcohol-induced sexual dysfunction • F10.282 Alcohol dependence with alcohol-induced sleep disorder • F10.288 Alcohol dependence with other alcohol-induced disorder • F10.29 Alcohol dependence with unspecified alcohol-induced disorder
Example of New Code Set • O35 Maternal care for known or suspected fetal abnormality and damage • Includes: the listed conditions in the fetus as a reason for hospitalization or other obstetric care to the mother, or for termination of pregnancy • Code also any associated maternal condition • Excludes1: encounter for suspected maternal and fetal conditions ruled out (Z03.7-) • One of the following 7th characters is to be assigned to each code under category O35. 7th character 0 is for single gestations and multiple gestations where the fetus is unspecified. 7th characters 1 through 9 are for cases of multiple gestations to identify the fetus for which the code applies. The appropriate code from category O30, Multiple gestation, must also be • ICD-10-CM Tabular Page 1025 2010 • assigned when assigning a code from category O35 that has a 7th character of 1 through 9. • 0 not applicable or unspecified • 1 fetus 1 • 2 fetus 2 • 3 fetus 3 • 4 fetus 4 • 5 fetus 5 • 9 other fetus • O35.0 Maternal care for (suspected) central nervous system malformation in fetus • O35.1 Maternal care for (suspected) chromosomal abnormality in fetus • O35.2 Maternal care for (suspected) hereditary disease in fetus • O35.3 Maternal care for (suspected) damage to fetus from viral disease in mother • O35.4 Maternal care for (suspected) damage to fetus from alcohol • O35.5 Maternal care for (suspected) damage to fetus by drugs • O35.6 Maternal care for (suspected) damage to fetus by radiation • O35.7 Maternal care for (suspected) damage to fetus by other medical procedures • O35.8 Maternal care for other (suspected) fetal abnormality and damage • O35.9 Maternal care for (suspected) fetal abnormality and damage, unspecified
Example of New Data Collection • R40.2 Coma • Coma NOS; Unconsciousness NOS • Codes first any associated: • coma in fracture of skull (S02.-) • coma in intracranial injury (S06.-) • The appropriate 7th character is to be added to each code from subcategory R40.21-, R40.22-, R40.23-: • 0 unspecified time • 1 in the field [EMT or ambulance] • 2 at arrival to emergency department • 3 at hospital admission • 4 24 hours or more after hospital admission • A code from each subcategory is required to complete the coma scale • Note: These codes are intended primarily for trauma registry and research use but may be utilized by all users of the classification who wish to collect this information • R40.20 Unspecified coma • R40.21 Coma scale, eyes open • R40.211 Coma scale, eyes open, never • R40.212 Coma scale, eyes open, to pain • R40.213 Coma scale, eyes open, to sound • R40.214 Coma scale, eyes open, spontaneous
Coma • R40.22 Coma scale, best verbal response • R40.221 Coma scale, best verbal response, none • R40.222 Coma scale, best verbal response, incomprehensible words • R40.223 Coma scale, best verbal response, inappropriate words • R40.224 Coma scale, best verbal response, confused conversation • R40.225 Coma scale, best verbal response, oriented • R40.23 Coma scale, best motor response • R40.231 Coma scale, best motor response, none • R40.232 Coma scale, best motor response, extension • R40.233 Coma scale, best motor response, abnormal • R40.234 Coma scale, best motor response, flexion withdrawal • R40.235 Coma scale, best motor response, localizes pain • R40.236 Coma scale, best motor response, obeys commands
Coding Guidelines • Same – Look it up in the alphabetic, then check in the tabular • Same – Abbreviations • Same – Punctuation • Same – use of “and,” “with,” “see,” “see also” • Same – other and unspecified codes • Same – includes notes and inclusion terms • Same – etiology/manifestation (code first, use additional code, in disease classified elsewhere) • Same – must use all available characters • Same – conditions that are or are not an integral part of the disease process
Coding Guidelines • Same – Acute and Chronic conditions • Same – Late Effects (sequela) • Same – Human Immunodeficiency Virus (HIV) coding • Same – Treatment directed at malignancy • Same – Treatment of secondary site of maligancy • Same – Primary malignancy previously excised • Same – Admission/Encounter for chemo • Same – Hypertension • Same – Acute myocardial infarction • Same – Coding Pathologic Fractures…
Coding Guidelines • New – placeholder “x” if the code only has 4 or 5 characters, but needs a 7th character (e.g., initial/subsequent/sequela to injury), use an “x” in the blank spaces • Different – Exclude1 (never code it here) and Exclude2 (not included, if he has that code it separately) • New – Laterality • New – Coding pregnancy trimesters • New – Glasgow coma scale • New – Functional quadriplegia
Review ICD-10-CM • Diagnoses, not procedures • Very similar to ICD-9-CM diagnoses, volumes 1 and 2 (diagnosis index and tabular) • Up to 7 alphanumeric characters BOTTOM LINE: If you can code with ICD-9-CM, you can easily transition to ICD-10-CM
Summary • MHS is working on the transition • The transition will be most difficult for the soft-ware programs • ICD-10-CM is much better than ICD-9-CM • Coders will not have a problem transitioning from ICD-9-CM to ICD-10-CM.
Quiz • Take the quiz again =-)
Q&A • Questions? • Training • Who needs ICD-10-CM training? • When (e.g., 2 months prior)? • Intensity (e.g., 1 hour teleclass a day with 1 hour a day at work to do the assigned lessons)? • Format (e.g., train-the-trainer to come back to work to train you, teleclasses, one REALLY large class [400 students in an auditorium], good teacher sent to each site for a week)?