Download
1 / 1
10 likes | 20 Views
CONCORDANCE WITH COMPRESSION THERAPY IN THE TREATMENT OF VENOUS LEG ULCERS. Fidelis Machado MD 1 , Dheerendra Kommala MD 1 , Nathalie Dourdin PhD 2 , Sharon Welner PhD 2 and Yoonhee Choe PharmD MHS 1 1 ConvaTec, Skillman, New Jersey, USA

E N D
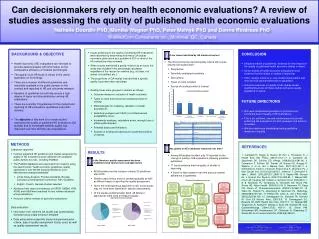
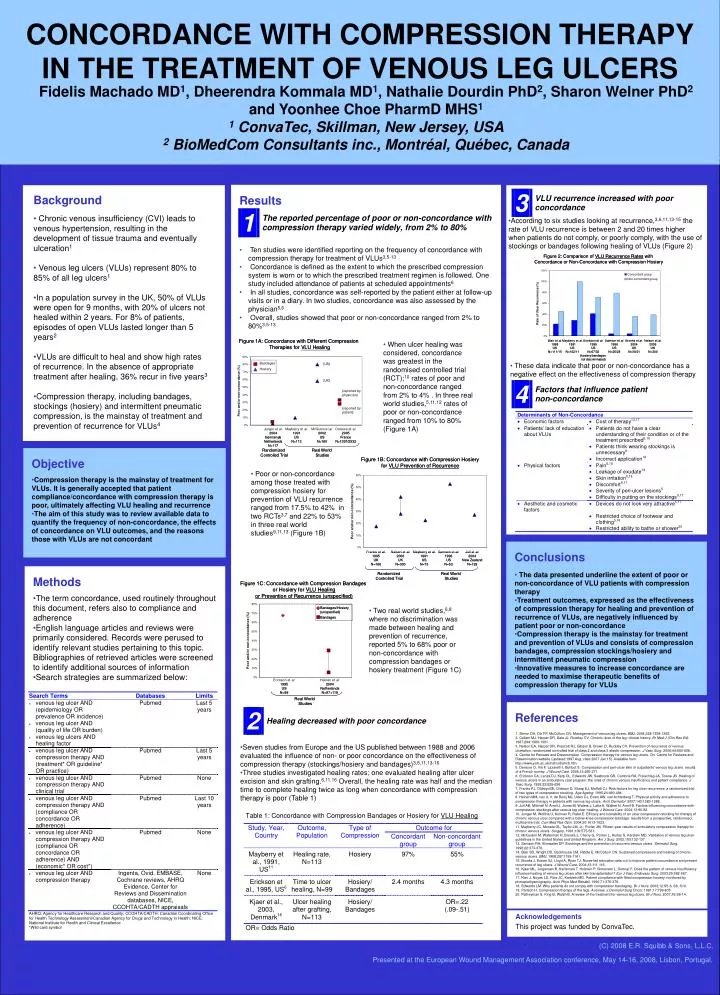
CONCORDANCE WITH COMPRESSION THERAPY IN THE TREATMENT OF VENOUS LEG ULCERS Fidelis Machado MD1, Dheerendra Kommala MD1, Nathalie Dourdin PhD2, Sharon Welner PhD2 and Yoonhee Choe PharmD MHS1 1 ConvaTec, Skillman, New Jersey, USA 2 BioMedCom Consultants inc., Montréal, Québec, Canada • Results • Ten studies were identified reporting on the frequency of concordance with compression therapy for treatment of VLUs3,5-13 • Concordance is defined as the extent to which the prescribed compression system is worn or to which the prescribed treatment regimen is followed. One study included attendance of patients at scheduled appointments6 • In all studies, concordance was self-reported by the patient either at follow-up visits or in a diary. In two studies, concordance was also assessed by the physician5,6 • Overall, studies showed that poor or non-concordance ranged from 2% to 80%3,5-13 • Background • Chronic venous insufficiency (CVI) leads to venous hypertension, resulting in the development of tissue trauma and eventually ulceration1 • Venous leg ulcers (VLUs) represent 80% to 85% of all leg ulcers1 • In a population survey in the UK, 50% of VLUs were open for 9 months, with 20% of ulcers not healed within 2 years. For 8% of patients, episodes of open VLUs lasted longer than 5 years2 • VLUs are difficult to heal and show high rates of recurrence. In the absence of appropriate treatment after healing, 36% recur in five years3 • Compression therapy, including bandages, stockings (hosiery) and intermittent pneumatic compression, is the mainstay of treatment and prevention of recurrence for VLUs4 • According to six studies looking at recurrence,3,6,11,13-15 the rate of VLU recurrence is between 2 and 20 times higher when patients do not comply, or poorly comply, with the use of stockings or bandages following healing of VLUs (Figure 2) • When ulcer healing was considered, concordance was greatest in the randomised controlled trial (RCT);10 rates of poor and non-concordance ranged from 2% to 4% . In three real world studies,5,11,12 rates of poor or non-concordance ranged from 10% to 80% (Figure 1A) • These data indicate that poor or non-concordance has a negative effect on the effectiveness of compression therapy • Objective • Compression therapy is the mainstay of treatment for VLUs. It is generally accepted that patient compliance/concordance with compression therapy is poor, ultimately affecting VLU healing and recurrence • The aim of this study was to review available data to quantify the frequency of non-concordance, the effects of concordance on VLU outcomes, and the reasons those with VLUs are not concordant • Poor or non-concordance among those treated with compression hosiery for prevention of VLU recurrence ranged from 17.5% to 42% in two RCTs3,7 and 22% to 53% in three real world studies9,11,13 (Figure 1B) • Conclusions • The data presented underline the extent of poor or non-concordance of VLU patients with compression therapy • Treatment outcomes, expressed as the effectiveness of compression therapy for healing and prevention of recurrence of VLUs, are negatively influenced by patient poor or non-concordance • Compression therapy is the mainstay for treatment and prevention of VLUs and consists of compression bandages, compression stockings/hosiery and intermittent pneumatic compression • Innovative measures to increase concordance are needed to maximise therapeutic benefits of compression therapy for VLUs • Methods • The term concordance, used routinely throughout this document, refers also to compliance and adherence • English language articles and reviews were primarily considered. Records were perused to identify relevant studies pertaining to this topic. Bibliographies of retrieved articles were screened to identify additional sources of information • Search strategies are summarized below: • Two real world studies,6,8 where no discrimination was made between healing and prevention of recurrence, reported 5% to 68% poor or non-concordance with compression bandages or hosiery treatment (Figure 1C) References 1. Simon DA, Dix FP, McCollum CN. Management of venous leg ulcers. BMJ. 2004;328:1358-1362. 2. Callam MJ, Harper DR, Dale JJ, Ruckley CV. Chronic ulcer of the leg: clinical history. Br Med J (Clin Res Ed). 1987;294:1389-1391. 3. Nelson EA, Harper DR, Prescott RJ, Gibson B, Brown D, Ruckley CV. Prevention of recurrence of venous ulceration: randomized controlled trial of class 2 and class 3 elastic compression. J Vasc Surg. 2006;44:803-808. 4. Centre for Reviews and Dissemination. Compression therapy for venous leg ulcers. On. Centre for Reviews and Dissemination website {updated 1997 Aug; cited 2007 Jan 15}. Available from: http://www.york.ac.uk/inst/crd/ehcb.htm 5. Dereure O, Vin F, Lazareth I, Bohbot S. Compression and peri-ulcer skin in outpatients' venous leg ulcers: results of a French survey. J Wound Care. 2005;14:265-271. 6. Erickson CA, Lanza DJ, Karp DL, Edwards JW, Seabrook GR, Cambria RA, Freischlag JA, Towne JB. Healing of venous ulcers in an ambulatory care program: the roles of chronic venous insufficiency and patient compliance. J Vasc Surg. 1995;22:629-636. 7. Franks PJ, Oldroyd MI, Dickson D, Sharp EJ, Moffatt CJ. Risk factors for leg ulcer recurrence: a randomized trial of two types of compression stocking. Age Ageing. 1995;24:490-494. 8. Heinen MM, van d, V, de Rooij MJ, Uden CJ, Evers AW, van Achterberg T. Physical activity and adherence to compression therapy in patients with venous leg ulcers. Arch Dermatol. 2007;143:1283-1288. 9. Jull AB, Mitchell N, Arroll J, Jones M, Waters J, Latta A, Walker N, Arroll B. Factors influencing concordance with compression stockings after venous leg ulcer healing. J Wound Care. 2004;13:90-92. 10. Junger M, Wollina U, Kohnen R, Rabe E. Efficacy and tolerability of an ulcer compression stocking for therapy of chronic venous ulcer compared with a below-knee compression bandage: results from a prospective, randomized, multicentre trial. Curr Med Res Opin. 2004;20:1613-1623. 11. Mayberry JC, Moneta GL, Taylor LM, Jr., Porter JM. Fifteen-year results of ambulatory compression therapy for chronic venous ulcers. Surgery. 1991;109:575-581. 12. McGuckin M, Waterman R, Brooks J, Cherry G, Porten L, Hurley S, Kerstein MD. Validation of venous leg ulcer guidelines in the United States and United Kingdom. Am J Surg. 2002;183:132-137. 13. Samson RH, Showalter DP. Stockings and the prevention of recurrent venous ulcers. Dermatol Surg. 1996;22:373-376. 14. Blair SD, Wright DD, Backhouse CM, Riddle E, McCollum CN. Sustained compression and healing of chronic venous ulcers. BMJ. 1988;297:1159-1161. 15. Brooks J, Ersser SJ, Lloyd A, Ryan TJ. Nurse-led education sets out to improve patient concordance and prevent recurrence of leg ulcers. J Wound Care. 2004;13:111-116. 16. Kjaer ML, Jorgensen B, Karlsmark T, Holstein P, Simonsen L, Gottrup F. Does the pattern of venous insufficiency influence healing of venous leg ulcers after skin transplantation? Eur J Vasc Endovasc Surg. 2003;25:562-567. 17. Kiev J, Noyes LD, Rice JC, Kerstein MD. Patient compliance with fitted compression hosiery monitored by photoplethysmography. Arch Phys Med Rehabil. 1990;71:376-379. 18. Edwards LM. Why patients do not comply with compression bandaging. Br J Nurs. 2003;12:S5-6, S8, S10. 19. Partsch H. Compression therapy of the legs. A review. J Dermatol Surg Oncol. 1991;17:799-805. 20. Palfreyman S, King B, Walsh B. A review of the treatment for venous leg ulcers. Br J Nurs. 2007;16:S6-14. • Seven studies from Europe and the US published between 1988 and 2006 evaluated the influence of non- or poor concordance on the effectiveness of compression therapy (stockings/hosiery and bandages)3,6,11,13-16 • Three studies investigated healing rates; one evaluated healing after ulcer excision and skin grafting.6,11,16Overall, the healing rate was half and the median time to complete healing twice as long when concordance with compression therapy is poor (Table 1) Acknowledgements This project was funded by ConvaTec. . (C) 2008 E.R. Squibb & Sons, L.L.C. Presented at the European Wound Management Association conference, May 14-16, 2008, Lisbon, Portugal.