Download
1 / 20
200 likes | 341 Views
Implementation of screening and brief intervention in accident and emergency departments: challenges and solutions Paolo Deluca, PhD Institute of Psychiatry, King’s College London.

E N D
Implementation of screening and brief intervention in accident and emergency departments: challenges and solutions Paolo Deluca, PhDInstitute of Psychiatry, King’s College London A&E St. Mary’s 'Scientia Vincit Timorem'
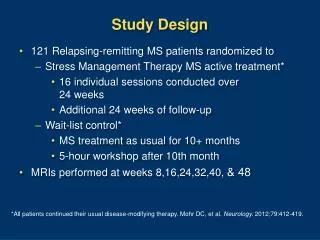
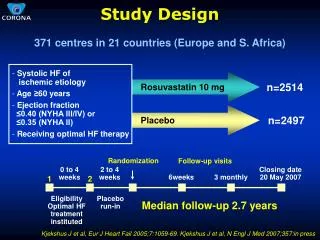
AED study design • 9 AEDs, 3 regions (NE, London, SE) • 3 screening approaches (M-SASQ, SIPS-PAT, FAST) • 3 intervention approaches • Patient information leaflet • Brief advice (5 min) • Referral to Alcohol Health Worker BLC (20 min) • 1,179 patients (131 each) • Baseline research interview • 6 & 12 month follow-up research interview • Attitudes, barriers and facilitators factors
Attitudes, barriers and facilitators factors • The Shortened Alcohol and Alcohol Problems Questionnaire (SAAPPQ) • Training and experience in dealing with AUDs • Multiple choice assessment • Feedback questions • Implementation questionnaire • T1 vs T2 vs T3
How do we assess implementation? • Number screened, positives, received intervention • Factors supporting implementation • Factors impeding implementation • Impact: individual, service, costs and benefits • Acceptability: patient, practitioner, commissioner • Sustainability
Overview recruitment • Recruited 9 A&Es – Royal Ham., St Thomas, King’s, North Mid, Central Mid, Newcastle Gen, Darlington Mem., Hexham, South Tyneside. • Trained 250 (range 5-84) staff (nurses and consultants) • Recruiting participants from April 08 to April 09 • 1202 (102%)
Training A&E staff • On site training to small and large groups delivered by RA & AHW • 1 to 2 hrs for screening and BA including role play • No BLC training • Overall positive feedback on training. Research elements and Units are usually the challenging parts of the training • Most welcomed receiving training • Adequate space, staff availability, “on call”, turnover, time and implementation issues slowed training • Booster sessions, launch events, shadowing staff first few weeks
SAAPPQ • Staff’s attitude and motivation • SAAPPQ assesses differences in five areas: • Role adequacy • Role legitimacy • Motivation • Task-specific self-esteem • Work satisfaction
SAAPPQ between groups(preliminary findings) • Overall A&E staff score significantly better than PHC and CJS staff respectively (p = .000) • Role security • Staff in A&Es score significantly better that PHC and CJS respectively • Therapeutic commitment • Staff in A&Es score significantly better that PHC and CJS respectively
SAAPPQ within group (T1 vs T2)(preliminary findings) • Overall A&E staff score significantly better than before the training (p = .000). In particular: • Role security • Staff in A&Es score significantly better after training (p = .02) • Therapeutic commitment • Staff in A&Es score significantly better after training (p = .000)
A&E Implementation issues • Protocol: Leaflet-eligibility-screening-informed consent-baseline-intervention • Ideally delivered by same person (except BLC) in practice divided by triage/nurses and doctors • Strong local lead (champion) • Consent and contact details put some participants off • Workload/time • Staff turnover (eg August) • Easily forget training if start is delayed • Tendency of targeting dependent drinkers • Weekly support
Implementation issues for screening and BI • Workload/time • Language/communication barriers • Too intoxicated patients • Patients not wanting to engage • Time/staffing/resources • Unwillingness of patients to engage • Space/privacy to deliver intervention • No dedicated alcohol health worker/internal A&E service to refer to. • Dealing with presenting problem
Changes to improve recruitment • Extra support to staff • Incentives (MHRN) • Deployment of Alcohol Health Workers to conduct also screening, BA and research assistants to support baseline activities
Conclusions • Prevalence of AUDs reflect previous studies in these settings • Patients are more willing to receive an intervention than previous studies • Overall staff in these settings are keen to be trained, have positive attitude and motivation • However, limited time, workload, lack of privacy and turnover are limiting implementation • Need for support or dedicated AHWs