Download

1 / 28
380 likes | 869 Views
Thrombotic disorders. virchow ´S Triad. Alterations in blood flow ( ie,stasis ) Vascular endothelial injury Alterations in the constituents of the blood( ie , inherited or acquired hypercoagulable state ). Classification of thrombophilias. Inherited protein C and S

E N D
virchow´S Triad • Alterations in blood flow (ie,stasis) • Vascular endothelial injury • Alterations in the constituents of the blood(ie, inherited or acquired hypercoagulable state )
Classification of thrombophilias • Inherited • protein C and S • Antithrombin III • FVL mutation 12-19% • Methyltetrahydrofolatereductase mutation (MTHFR) • Prothrombin G20210A mutation.6-8% ( PGM) • Antiprotein Z deficiency. • Dysfibrinogenemia . • Acquired • lupus anticoagulant • Anticardiolipin antibodies • Activated protein C resistance • Hyperhomocystinemia
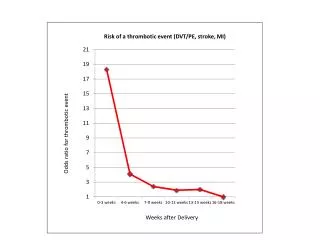
Acquired disorders • Malignancy • Presence of a central venous catheter • Surgery , especially orthopedic • Trauma • Pregnancy • Oral contraceptives • HRT • Tamoxifen, thalidomide, Lenalidomide • Immobilization • Congestive failure • Polycytemiavera, thrombocythemia • Paroxysmal nocturnal hemoglobinuria • Inflammatory bowel disease • Nephrotic syndrome
Anatomic risk factors for DVT • Paget-Schroetter syndrome . • May-Thurner syndrome (iliac vein compression ). • Inferior vena cava abnormalities (Agenesis, Hypoplasia, or Malformation ) • 9
Elevated clotting factors • VIII:C>150 percent • XI:A>121 percent • IX:A>129 percent • TAFI>122 percent(thrombin activatable fibrinolysis inhibitor • Interleukin 8>8.2 pg/ml
Thrombotic disorders Laboratory tests for the diagnosis Family history of thrombosis Family history of thrombophilias Prior unexplained fetal death Prior sever early onset preeclampsia (<34 weeks) Prior sever IUGR Prior sever placental insufficiency abnormal Doppler velocimetry abnormal placental histology oligohydramnious
APOadverse pregnancy outcome Maternal venous thromboembolism arterial thrombosis sever preeclampsia Placental thrombosis and infarcts abruptio Fetal recurrent miscarriage sever IUGR Fetal demise Stroke
Factor V Leiden • FV Leiden is a mutation gene which leads to phenotype of APCR(activated protein C resistance). • Prothrombin G21210A is mutation in factor II gene. • Antithrombin III(AT): heparin cofactor.{ type I and type II defects. • AT antigen measurement by ELISA is normal in type II AT deficiency.as many as 28% .and will be missed. • Protein C . • Protein S . • Dysfibrinogenemia. may cause bleeding or thrombosis .diagnosis can be confirmed by study of fibrinogen antigen. • Factor VIII activity elevation . • Factor IX and XI elevations . • Antiphopholipid antibodies (LA ,ACA ,ß2-glycoprotein I) . • Hyperhomocysteinemia .
Variables affecting tests • Pregnancy . • Oc pills . • HRT. • Thrombotic event . • Systemic illness. • Heparin or warfarin
APS clinical feature • Thrombosis ,PE ,TIA , • Thrombocytopenia. • Migraine headache • Transverse myelitis • Chorea • Syndromes resembling multiple sclerosis
Management of thrombosis in APS • Heparin should be continued for at least 5 days, and should be overlap with warfarin
Thrombophilias ,perinatal stoke. And cerebral palsy • Perinatal arterial ischemic stroke (PAS). • Occurring between 28 weeks and 28 days of post natal life, • Usually occurs before about 72 hours of postnatal life • Focal arterial infarction of brain and cerebral venous thromboses .unilateral or bilateral PAS. • MRI or CT Scan. • Ultrasonography is not a sensitive detector of stoke.
Clinical feature of PAS • Hypotonia • Apneas • Neonatal seizures intractable to medical therapy. • Asymmetry of movement • The diagnosis is 4 to 8 months. • Delayed language development • Majority of children who had cerebral palsy caused by perinatal stroke were not recognized to be affected in the newborn period.
Pregnancy related stroke in the mother • Risk factors : infection ,migraine ,thrombophilias ,APS ,SLE ,heart disease ,pre-eclampsia ,diabetes ,smoking ,obesity ,older age ,prolonged bed rest .C/S . In the fetus .high hematocrit ,injury to neck vessels .newborn dehydration ,hypotension ,infection ,intravascular catheters ,
Combination of clinical outcomes that should prompt a consideration of underlying thrombophilias • Abruption Retroplacentalhematom Recent villous infarction Intruterine growth restriction preeclampsia
The use of unfractionated heparin and low molecular weight heparin in pregnancy • Warfarin is generally avoided during pregnancy and is safe to use postpartum . • UH mean molecular weight 15000 d • aPTT >1.5 to 2.5mean control . • thromboprophylaxis with UH in first trimester 5000iu BID ,second trimester 7500iu BID ,in third trimester 10000iu BID • Acute Therapeutic dose of UH in pregnancy: initial bolus 80 units/kg, and continuous infusion 16 to 18 units/kg/h for 5 day, then converted to intermittent subcutaneous heparin • Patients with mechanical cardiac valves should receive therapeutic anticoagulation during pregnancy .
LMWH • Mean molecular weight 500 d ,do not cross the placenta in any trimester. • Anti Xa activity must be measured. • Are excreted renally. • Twice daily dosing may be required . • Osteoporosis and thrombocytopenia may be less • Therapeutic range for anti Xa level is 0.5 to 1.0IU/mL • Monitoring levels every 2 to 4 weeks .
Intrapartum management • 6 hours after vaginal delivery and 12 hours after C/S prophylaxis is resumed. • 12 to 24 hours before discontinuing LMWH for regional anesthesia . • Some clinicians switch patients on LMWH to UH 10000units every 12 hours at approximately 36 weeks gestation. • For high risk patients on therapeutic intravenous UH therapy stopped 3 to 6 hours before delivery . • After delivery full anticoagulant with coumadin started concomitantly . • Initial dose of coumadin should not exceed 5 mg . • Postpartum anticoagulant continue for 6 to 8 weeks and for recent VTE treatment with coumadin continued for 3 to 6 months.
Prosthetic cardiac valves in pregnancy • ACOG and ACC recommendation : enoxaparin sodium patients should be started on 1 mg/kg every 12 hours and to achieve peak anti-Xa levels 1.0-1.5 IU/mL The addition of aspirin 82mg/d. was also felt to be prudent.
Time of delivery • Fetal assessment with NST beginning at >36 weeks of gestation and delivery at 39 weeks of gestation in the abernce of preeclampsia ,abruption ,IUGR . • If obstetrical complications are present ,fetal surveillance should be earlier .
inherited dysfibrinogenemia • Silent 55% • Hemorrhagic 25% • Thrombotic diathesis 10-20% • Thrombotic and bleeding 2% • A rare cause of thrombophilias 0.8% • The prevalence of thrombosis (venous/arterial) • among patients with dysfibrinogenemia is around 10 to 20% .
Acquired disorders • Liver disease • Renal carcinoma • Isotretinoin therapy • Biliary obstruction • Acute DIC • Cryofibrinogenemia is seen in autoimmune disorders ,malgnancy ,thrombotic disorders ,and infections (hepatitis C ) and DIC .symptoms include sensitivity to cold ,Raynaudsphenomen ,purpura ,urticaria ,skin ulcerations or gangrene , and thrombosis .
Diagnosis and treatment • PT • TT • aPTT • Fibrinogen replacement prior to surgery >100 mg/DL • Pregnancy: weekly measurement and requirement from 2 g twice weekly during the first trimester to 5 g three to four times per week at term. • During labor: fibrinogen level 150 to 200 mg/dl. • After 24 hours. fibrinogen level >50 mg/dl should be maintained .
Available treatment modalities • Cryoprecipitate and FFP :one unit (10 to 15 ml) contains approximately 200 to 400 mg fibrinogen .each unit raises fibrinogen 7 to 10 mg/dl with half life of two to four days . • 1-2 unit of cryo per 10 kg body weight. • Maintenance dose of approximately one third of the initial dose is infused daily for two to three weeks following major surgery. • Complications : allergic reactions, transmission of infection ,and thrombosis , • Fibrinogen concentrate: • Dose(mg)=target fibrinogen(mg/dl)-measured fibrinogen level +1.7 xbody weight(kg)